Atrial Fibrillation Answered in 8 Steps
In this video, Dr Nijjer explains Atrial Fibrillation (“AF”), a common heart condition which causes palpitations. It is an important condition to diagnose because if untreated, it can cause strokes.

What is AF?
Atrial Fibrillation is an arrhythmia that affects the upper two chambers of the heart – the atria. It is increasingly common and, in those over the age of 70 years of age, can be present in almost 10% of the population.
The most common causes of Atrial fibrillation are age, hypertension (high blood pressure), alcohol consumption and thyroid disorder.
When patients develop atrial fibrillation, they will feel their heart is jumping uncontrollably. Some patients may feel dizzy or light headed. Others may feel only a slight change in their well-being. Others can feel a terrible fast racing heart.
What types of AF are there?
The symptoms of AF may come and go, and hence we refer to this as Paroxysmal AF. In some patients, the AF may be present all of the time (referred to as Persistent AF).
We may be able to give therapy to restore the normal heart beat (called Sinus rhythm).
In some patients, we cannot restore normal activity and so this is called Permanent AF.
AF increases the risk of stroke
While the patient is in AF, the heart loses some of it’s efficiency. The atria have disorganised electrical activity but have no effective contractions. This means blood swirls around slowly within the atria and this means it can form clots. These clots can move out of the heart and travel to other parts of the body. If they travel to the brain, they can cause devasting stroke.
Patients with AF are assessed according to a number of risk scores which try to predict the likelihood of stroke. The most common risk score is called the CHA₂DS₂VASc score – and those patients with a score of more than 2, will be recommended to talk a blood thinning medication.


Medications to thin the blood
Not so long ago, the standard of care was to give a drug called warfarin. This is highly effective at reducing stroke but has the disadvantage of requiring different doses on different days and frequent blood tests to measure the blood thickness (called INR).
Warfarin has now been supplanted by the ‘DOAC’ (Direct Oral Anticoagulation’) class of drugs, of which the principle ones used are Apixaban (taken twice a day), Rivaroxaban and Edoxaban (both taken once a day, with food). These drugs are as effective as warfarin, but cause less bleeding and do not require blood tests. Therefore they have now become the standard of care.

Detecting AF
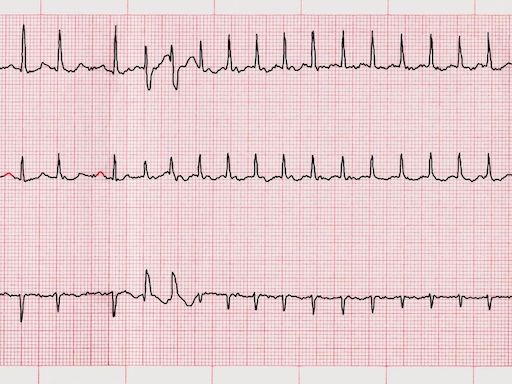
If an ECG (Electrocardiogram) is performed at the time of the symptoms, we may capture an irregular heart beat. However, ECGs are only a snapshot of the heart and may not capture the AF as it tends to come and go. In this case, we may ask you to wear a Holter monitor.
While the heart is in AF, the atria have disorganised electrical activity and we can see there is irreguar gaps between the heart beats.
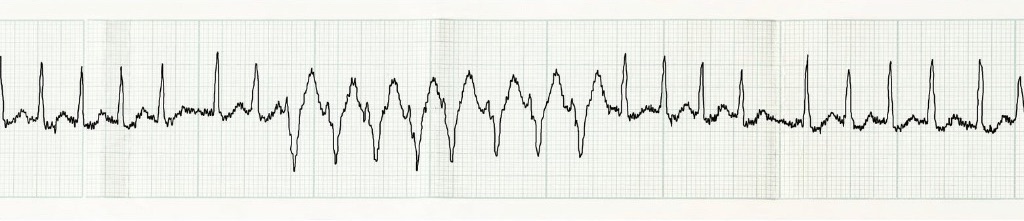
AF with Fast Heart Beats
In some cases, the heart beats can be too fast. If this is the case, we need to give medications that can slow down the heart beat. This can include beta-blockers such as Bisoprolol, calcium-channel inhibitors such as Diltiazem or drugs like Digoxin. In some cases, multiple combinations of drugs will be needed. In those patients who have recurrent paroxysms of AF, we may use drugs such as Flecainide or Amiodarone to reduce the events.
Amiodarone is highly effective but has risks of side-effects. It can cause problems with the lungs, liver and thyroid. Prolonged use may also cause skin discolouration (a blue tinge can develop). Those on the medication should avoid sunbathing as it the skin is sensitive and should have a Chest X-ray test as well as regular blood tests every year.
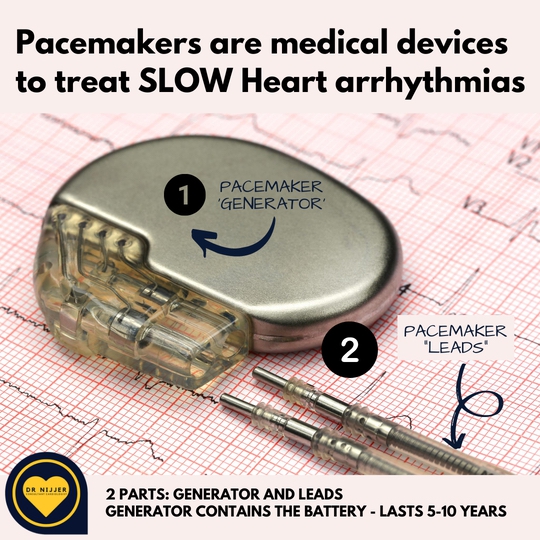
AF with Slow Heart Beats
In patients in whom the AF is causing a very slow heart beat, then a Pacemaker may be needed. This is particularly the case if the patient is having fainting episodes. It may also be used if the heart moves quickly between fast and slow heart beats. In this situation, medications can help slow down the fast heart beats, but if the heart is too slow, then the pacemaker will prevent it becoming too slow.
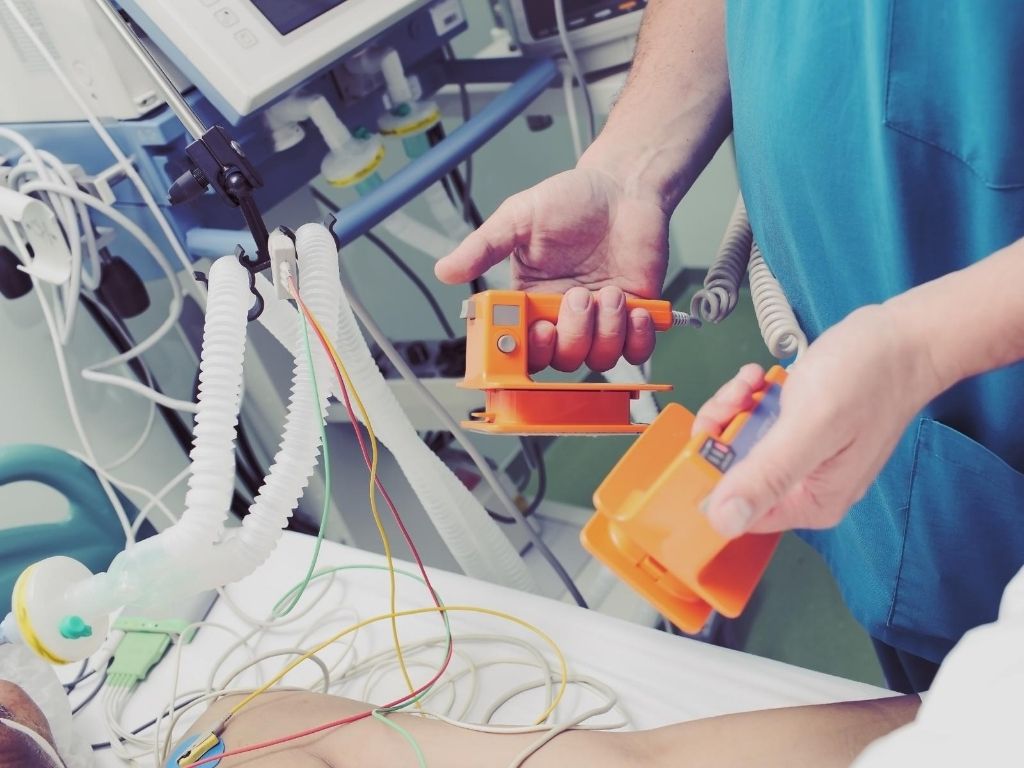
DC Cardioversion
In patients who have new onset AF, then we may consider performing a DC Cardioversion. This is a procedure performed under general anaesthesia and may require a period of 6 weeks of blood thinners before it can be performed. This reduces the risk of clot being within the heart. We may perform a telescope echocardiogram test, called a transoesophageal echocardiogram (TOE), to ensure there are no clots within the heart.
Once this is done and the patient is deeply asleep, a controled electric shock is delivered to the chest. This causes the heart’s electrical signals to be reset and normal Sinus rhythm to be restored. It is essential for patients to continue to take their blood thinning medications after the procedure because there remains a risk of clot.
AF Ablation
In patients who have recurrent symptoms of atrial fibrillation despite good medical therapy, then we may offer them an Ablation procedure. This is a complex procedure performed within a Hospital with the appropriate facilities and may be performed with or without sedation depending on the type of ablation being performed.
Special catheters are placed within the atria and the pulmonary veins and very careful selective burns are made within the heart to stop the abnormal electrical signals. The success of AF ablation can vary according to the complexity of the case and AF may recur in the first few months after the procedure while the heart recovers. In some patients a second or third ablation may be required to fully remove the AF.


Cardiac Testing For Atrial Fibrillation
ECG
An electrocardiogram (ECG) is essential to confirm the diagnosis but may not capture the AF. Wearing a Holter monitor will increase the likelihood of making the diagnosis and the longer the duration of the monitor, the better the chance of making the diagnosis.
Echocardiogram
An ultrasound of the heart will show us if there is any weakness or damage. Heart valves may be leaking and need monitoring over time. Mitral regurgitation (leaking mitral valve) is commonly associated with atrial fibrillation. The left atrium may also be dilated.
C
Cardiac Blood Tests
There are no routine blood tests that can detect AF, but we will check your thyroid function and kidney function. We will also look for hypertension (high blood pressure) as this is a common cause of AF.
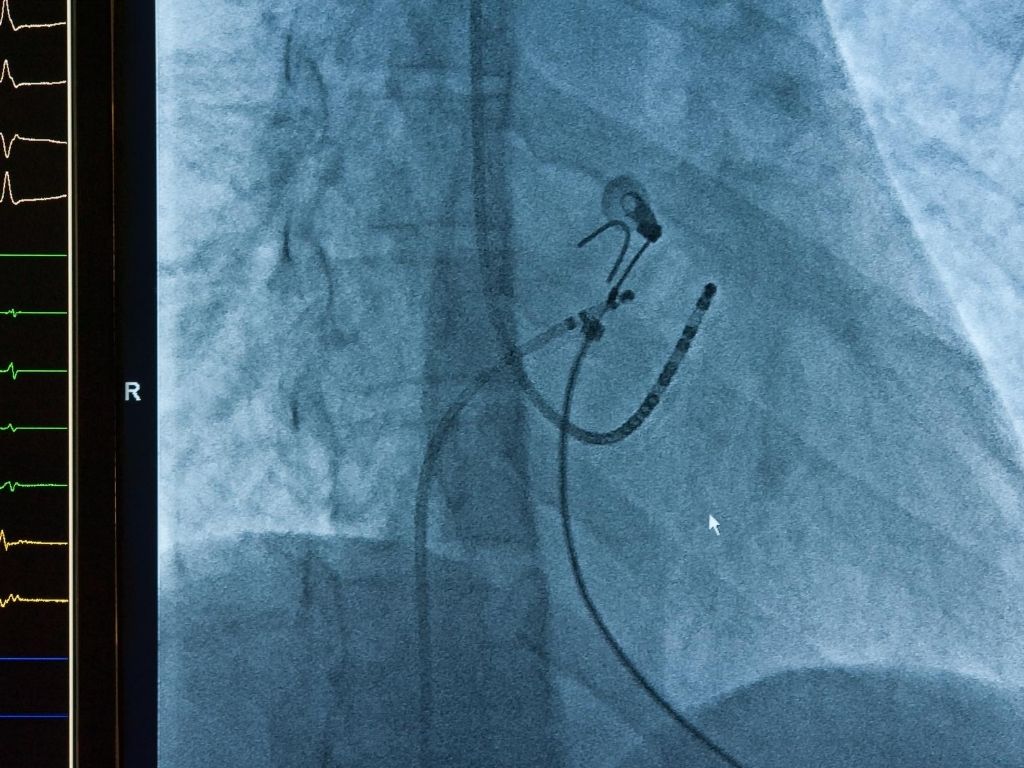
Invasive Studies
In some patients will require invasive electrophysiology studies in order to map the abnormal electrical pathways causing the arrhythmia. An ablation can burn away the cause of the problem but you may require more than one procedure to have complete success.
A patient's perspective
I kept having palpitations and the feeling that my heart was trying to jump out of my chest. I had been seen by my GP and they referred me to Dr Nijjer. He quickly diagnosed AF using an ECG and started me on medication which controlled it. I needed blood thinners to stop me from having a stroke. I’m so grateful to Dr Nijjer for using the newer drugs so that I could avoid using Warfarin. My palpitations are much better now.
Help Your Heart
If you have any concerns regarding your heart health, then please seek a referral to Dr Nijjer.
Call the Team: Amy, Monika, Charlotte, Erin or Grace:
0203 9838 001
Email: Secretary@DrNijjer.com
Dr Nijjer can be seen at :
68 Harley Street, London, W1G 7HE
Dr Nijjer also practices at Cromwell Hospital, Wellington Hospital, BUPA Clinics, BMI Syon Clinic as well as Imperial Private Healthcare.
