Procedure — Coronary Intervention
Coronary Angiography
& Angioplasty
Coronary angiography is the gold-standard test for assessing the heart arteries. When a significant blockage is found, angioplasty — opening the artery with a balloon and stent — can relieve symptoms and prevent a heart attack.

The Gold-Standard Test
Coronary Angiography
Coronary angiography is the definitive test for assessing the coronary arteries — the vessels that supply blood to the heart muscle. It is typically performed when non-invasive tests suggest the possibility of coronary artery disease, or when symptoms of chest pain or breathlessness remain unexplained.
The procedure is performed in a hospital catheter laboratory, usually as a day case. Light sedation may be used but a general anaesthetic is not required. You will fast beforehand, though a prolonged fast is not necessary — Dr Nijjer will advise on the exact duration.
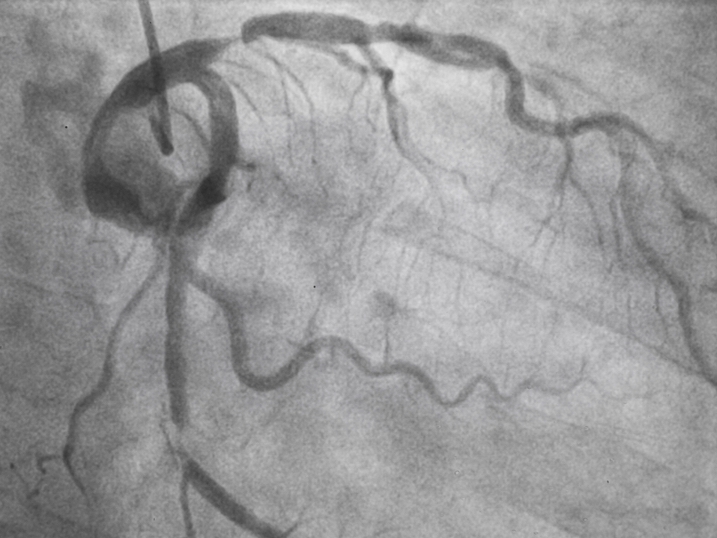
A small tube (catheter) is passed to the heart arteries via the wrist (radial approach) or, less commonly, the upper groin (femoral approach). X-ray contrast dye is injected into the coronary arteries so they can be seen clearly on screen. A typical study takes 10–15 minutes.
Step by Step
How the Procedure Works
Preparation & Access
A small puncture is made at the wrist (radial) or groin (femoral). A thin plastic sheath is inserted into the artery.
Catheter Placement
A flexible catheter is guided through the artery to the opening of each coronary artery. You will not feel this.
Contrast & Imaging
X-ray contrast dye is injected. The coronary arteries show up on a live X-ray screen, revealing any narrowings or blockages.
Assessment
Dr Nijjer assesses each artery, measuring narrowings and using pressure wires or imaging catheters where needed.
Treatment or Discharge
If a stent is needed it can often be placed at the same sitting. Most patients go home the same day.
Indications
When Is Angiography Needed?
Angiography is recommended when there is a clinical concern about blood supply to the heart — whether from symptoms, abnormal test results, or an acute presentation.
Stable Angina
Chest discomfort during exertion caused by a significant narrowing restricting blood flow. Angiography confirms the location and severity. Stenting can relieve symptoms where medications are insufficient.
Heart Attack (STEMI / NSTEMI)
A sudden complete or partial blockage of a coronary artery requires urgent angiography to identify and open the blocked vessel, limiting permanent damage to the heart muscle.
Abnormal Non-Invasive Tests
A positive exercise stress test, stress echocardiogram, or CT coronary angiogram may suggest significant disease that warrants direct assessment and potential treatment.
Treatment
Coronary Angioplasty & Stenting
When there is significant ischaemia (insufficient blood supply) or an acute blockage, the narrowing can be treated by placing a coronary stent — a small metallic mesh structure that holds the artery open.
A thin guidewire is first advanced through the narrowing. A balloon catheter is then passed over the wire and inflated to compress the plaque. The stent — crimped onto the balloon — is deployed and expands to scaffold the artery wall. The balloon is removed, leaving the stent permanently in place.
Dr Nijjer uses pressure wires and intravascular imaging to ensure each stent is placed precisely where it will deliver the greatest benefit. In most cases the procedure is done under local anaesthetic with light sedation, through the wrist, and patients go home the same day. Complex cases may require an overnight stay.

Dr Nijjer's Specialist Expertise
Advanced Techniques
Not all angioplasty procedures are straightforward. Complex cases — heavily calcified arteries, long diffuse disease, or multi-vessel involvement — require specialist skills and technology. Dr Nijjer is trained and experienced in the full range of advanced coronary intervention techniques.

Physiology
iFR & Pressure Wire
iFR (Instantaneous wave-Free Ratio) is a pressure wire measurement that tells Dr Nijjer whether a narrowing is actually restricting blood flow — and therefore whether a stent will help. Dr Nijjer co-developed this technology, which is now used in tens of thousands of patients worldwide and embedded in international guidelines.
Imaging
IVUS & OCT
Intravascular Ultrasound (IVUS) and Optical Coherence Tomography (OCT) are miniature imaging catheters that travel inside the coronary artery, providing cross-sectional images with far greater detail than angiography alone. They guide optimal stent sizing and confirm complete expansion.
Calcium Modification
Shockwave & Rotablation
Heavily calcified arteries cannot be adequately expanded with a standard balloon. Shockwave intravascular lithotripsy uses acoustic pressure waves to crack calcium. Rotational and orbital atherectomy use rotating burrs to debulk calcified plaque before stenting.
Calcium & Complex Disease
Laser Atherectomy
Excimer laser coronary atherectomy uses ultraviolet light energy to ablate calcified or fibrotic plaque and is used in complex anatomies where conventional techniques are limited.
Physiology
Angiography-Derived Physiology
Advanced computational analysis of the angiogram images can derive physiological pressure measurements without requiring a separate pressure wire, streamlining the assessment of multiple lesions in the same procedure.
Microvascular Disease
Microvascular Assessment
Some patients have angina despite no significant blockages. Dr Nijjer assesses the small coronary vessels for microvascular dysfunction, epicardial vasospasm, and myocardial bridging — conditions often missed by conventional angiography alone.
After Stenting
Medications After Your Procedure
Following coronary stent placement, blood-thinning medications are essential to prevent the stent from clotting. These must be taken reliably and must never be stopped without checking with Dr Nijjer first.
-
Aspirin 75mg daily
Prescribed to most patients with significant coronary artery disease. Reduces platelet activity and lowers the risk of further clot formation. Taken indefinitely.
-
Clopidogrel 75mg daily
The standard second antiplatelet agent after elective stenting. Combined with aspirin to prevent stent thrombosis. Usually continued for 12 months, sometimes longer.
-
Ticagrelor or Prasugrel
Used after a heart attack in place of clopidogrel. More potent antiplatelet effect reduces the risk of further events in patients who have experienced an acute coronary syndrome.
If antiplatelet medications are missed, a stent can clot suddenly (stent thrombosis) — a life-threatening emergency. If another doctor suggests stopping these medicines before a procedure, they should consult with Dr Nijjer first.

I had been having central chest tightness for some time. I called Dr Nijjer and saw him straight away. He organised tests showing I likely had blocked arteries. Because I kept having chest pain, Dr Nijjer performed an angiogram through my hand. I needed two stents and have felt so much better. I know I am in good hands.
Mr K.S.G.
Business Owner — Patient of Dr Nijjer
Related Conditions
Further Reading
Patient Questions
Stents & Angioplasty FAQs
The questions Dr Nijjer is asked most often about stents and angioplasty — what happens during the procedure, recovery, medications and life afterwards.
Medically reviewed by Dr Sukhjinder Nijjer, Consultant Interventional Cardiologist (GMC 6103417) · Last reviewed May 2026.
Jump to a question
- What is a coronary stent and how does it work?
- How long does a stent last?
- What is the recovery time after angioplasty?
- Can I exercise after having a stent?
- What medications will I need after a stent?
- Is a stent better than bypass surgery?
- Can arteries get blocked again after a stent?
- What is FFR or iFR during an angiogram?
- Are drug-eluting stents safe long-term?
- How risky is a coronary angiogram?
- Can I fly after having a stent?
- Stent vs medication for a heart attack — what is the difference?
What is a coronary stent and how does it work?
A coronary stent is a tiny mesh tube — usually 2 to 4 mm in diameter — delivered into a narrowed coronary artery on a balloon catheter. The balloon is inflated to crush the plaque against the artery wall and expand the stent, which then holds the artery open after the balloon is removed.
Modern stents are made of cobalt-chromium alloy and coated with a drug that prevents scar tissue from re-narrowing the artery — a drug-eluting stent. Once placed, the stent becomes incorporated into the artery wall within a few weeks. It is not removed — it stays for life.
How long does a stent last?
A well-placed modern drug-eluting stent typically lasts a lifetime in around 90% of patients. The stent itself does not wear out — it becomes permanently embedded in the artery wall.
The exceptions are restenosis (scar tissue regrowing inside the stent, mostly in the first year) and the development of new disease elsewhere in the coronary arteries. Both are minimised by taking medications consistently, controlling cholesterol and blood pressure aggressively, not smoking, and staying physically active. Stent durability is one of the biggest advances in cardiology over the past 20 years.
"It is remarkable how far stent technology has come. The drug-eluting stents we use today are extraordinarily thin and durable — patients who had stents 15 years ago and have taken their medications faithfully typically have stents that look pristine on repeat imaging. The technology works, and it lasts."
— Dr Sukhjinder Nijjer, Consultant Interventional Cardiologist
What is the recovery time after angioplasty?
For a planned (elective) angioplasty performed via the wrist, most patients are home the same day and back to normal light activity within 24 to 48 hours. Driving is usually allowed after a week, and most office workers return to work within a week or two.
Heavy lifting, vigorous exercise and contact sports should be avoided for about a week while the wrist access site heals. After an emergency angioplasty for a heart attack, recovery takes longer — typically 4 to 6 weeks before returning to full activity — and a structured cardiac rehabilitation programme is strongly recommended.
Can I exercise after having a stent fitted?
Yes — exercise is one of the most important things you can do after a stent. Most patients can resume walking immediately and build up to moderate aerobic activity within 2 to 4 weeks. After a heart attack, the progression is supervised through a cardiac rehabilitation programme.
Target around 150 minutes of moderate-intensity activity per week — brisk walking, cycling, swimming, gardening — plus two sessions of resistance work. Exercise improves heart function, lowers cholesterol, controls blood pressure and reduces the risk of a future event by around 25%. A properly placed stent does not restrict what you can eventually do.
I was part of the team that developed iFR — a method of measuring blood pressure across a coronary narrowing to determine whether it is actually restricting flow enough to cause symptoms and warrant a stent. Before physiology-guided stenting, we relied on visual estimates from angiograms alone, which we now know overestimates the need for treatment in many cases. iFR removes that uncertainty.
Modern stenting is remarkably precise. I use intracoronary imaging (IVUS and OCT) to see inside the artery at microscopic detail, ensuring the stent covers the lesion completely and expands fully. For heavily calcified arteries I use rotational atherectomy or shockwave intravascular lithotripsy to prepare the vessel before stenting. These techniques produce outcomes that would have been impossible a decade ago — and most patients go home the same day.
What happens during coronary angioplasty
The wrist (radial) is the preferred access point in most cases. A small tube (sheath) is inserted into the artery under local anaesthetic — most patients feel minimal discomfort.
A thin catheter is guided to the coronary arteries and contrast dye injected to visualise blockages. X-ray images are taken from multiple angles.
A pressure wire is passed across the narrowing to measure blood flow. This confirms whether stenting will genuinely improve blood supply to the heart muscle.
A small balloon opens the narrowing and a drug-eluting stent is deployed to hold it open permanently. Intracoronary imaging confirms optimal placement.
A final angiogram confirms blood flow is restored. The sheath is removed and the puncture site sealed. Most patients are monitored for a few hours and discharged the same day.
What medications will I need after a stent?
After a stent you will be on dual antiplatelet therapy (DAPT) — aspirin plus a second antiplatelet such as clopidogrel, ticagrelor or prasugrel — usually for 6 to 12 months, then aspirin (or a single antiplatelet) for life. These medications prevent clots forming on the stent surface.
You will also typically be prescribed a high-intensity statin regardless of your starting cholesterol level, and often a beta-blocker and an ACE inhibitor, particularly after a heart attack. Stopping antiplatelets early without medical advice is the single biggest preventable cause of stent failure. If you need surgery within the year, always inform the team about your stent. Read more about these medications →
Is a stent better than bypass surgery?
Neither is universally "better" — they are different tools for different patterns of disease. Stenting is less invasive, has a faster recovery, and is excellent for one- or two-vessel disease and for emergency treatment of heart attacks. Bypass surgery (CABG) tends to give more durable results for complex three-vessel disease, particularly in patients with diabetes or significantly impaired heart function.
For most modern patients with single or two-vessel disease, stenting is the first choice. For complex disease, the decision is made by a multidisciplinary heart team — interventional cardiologist plus cardiac surgeon — using the SYNTAX score and the patient's clinical features. The right pathway is the one that best fits your anatomy.
Can arteries get blocked again after a stent?
Yes, although it is uncommon with modern drug-eluting stents. In-stent restenosis — scar tissue growing inside the stent — occurs in around 5% of patients in the first year. Stent thrombosis — a sudden clot inside the stent — is rare, occurring in less than 1% of patients per year, and almost always linked to stopping antiplatelet medications too early.
New narrowings can also develop elsewhere in the coronary arteries as the underlying disease progresses — which is why aggressive risk-factor control matters even after a perfect stent result. Recurrent chest pain after a stent always deserves prompt re-evaluation.
What is FFR or iFR during an angiogram?
FFR (fractional flow reserve) and iFR (instantaneous wave-free ratio) are pressure-wire techniques used during a coronary angiogram to decide whether a narrowing is actually limiting blood flow to the heart muscle. The cardiologist threads a thin wire across the narrowing and measures the pressure drop as a precise number.
This matters because many narrowings look significant on X-ray but are not actually causing ischaemia — and stenting a non-significant lesion adds risk without benefit. FFR and iFR have transformed interventional cardiology over the past 15 years and are now embedded in major international guidelines.
A note on iFR from Dr Nijjer: The iFR technique was co-developed in my research group at Imperial College London and is now used in tens of thousands of procedures worldwide each year. Seeing a technology you helped create become part of everyday clinical practice — improving outcomes for real patients — is one of the most rewarding parts of an academic cardiology career. I use pressure-wire assessment routinely in my own practice to ensure every stenting decision is physiology-guided.
"I believe every patient deserves a stenting decision based on what the artery is actually doing, not just what it looks like on X-ray. Pressure-wire assessment takes a few minutes and changes the answer in a meaningful number of cases. It is one of the ways we protect patients from unnecessary procedures."
— Dr Sukhjinder Nijjer, co-developer of the iFR technique
Are drug-eluting stents safe long-term?
Yes — modern drug-eluting stents have been used for more than 20 years and the long-term safety data are excellent. The first-generation stents had a small late-stent thrombosis signal that is no longer seen with second- and third-generation devices, which use thinner struts and better drug formulations.
Long-term studies show drug-eluting stents are at least as safe as bare-metal stents and significantly better at preventing restenosis. The main long-term risk remains stopping antiplatelet medications early, which is why adherence to your prescribed regimen is so important.
How risky is a coronary angiogram?
A coronary angiogram is a very safe procedure in experienced hands. Serious complications — heart attack, stroke, major bleeding — occur in around 1 in 1,000 diagnostic angiograms, and slightly more when a stent is also placed.
The commonest minor complications are bruising at the wrist access site and a small reaction to the X-ray dye. Modern radial (wrist) access has roughly halved the bleeding risk compared with the older femoral (groin) approach and is now preferred for most patients. All risks are discussed individually at the time of consent.
Can I fly after having a stent?
Most patients can fly 2 weeks after a planned (elective) stent and 4 weeks after a stent for a heart attack, provided recovery has been straightforward. Some airlines require a medical clearance certificate after a cardiac procedure — always check before booking.
For long-haul flights, the additional concern is deep vein thrombosis from prolonged immobility. Stay hydrated, walk the aisle every couple of hours, use compression stockings if you are at higher DVT risk, and never stop your antiplatelet medications without speaking to your cardiologist first.
What is the difference between a heart attack treated with a stent and one treated with medication?
For most heart attacks — particularly the more serious type called STEMI — emergency stenting (primary PCI) is the gold-standard treatment and dramatically reduces death and heart muscle damage compared with medications alone. The UK has invested heavily in 24/7 primary PCI networks for exactly this reason.
Some smaller heart attacks (NSTEMI) can be managed initially with medications and have angiography within 72 hours rather than immediately. Stable angina, by contrast, is often best managed with medications first and angioplasty reserved for those who continue to have symptoms despite treatment. The right strategy depends on the type and severity of the event.
Concerned about your coronary arteries?
Dr Nijjer performs coronary angiography and complex angioplasty at Hammersmith Hospital and across his private clinic network. If you have been advised to consider angiography, or are experiencing chest pain, arrange an expert assessment today.