Heart Conditions — Arrhythmia
Atrial
Fibrillation
Atrial fibrillation is the most common sustained heart rhythm disorder, affecting around 10% of people over 70. It carries a significant stroke risk and is eminently treatable — but it must first be identified and properly assessed.

The Most Common Arrhythmia
What Is Atrial Fibrillation?
In a normal heart, a regular electrical signal from the sino-atrial node coordinates each heartbeat. In atrial fibrillation, the upper chambers (atria) fire chaotically — hundreds of times per minute — producing a rapid, completely irregular rhythm in the lower chambers (ventricles).
AF becomes increasingly prevalent with age, affecting approximately 10% of people over 70. The primary risk factors are advancing age, hypertension, alcohol use, thyroid disorders, obesity, and sleep apnoea.
Patients typically describe sensations of uncontrolled heart activity — fluttering, racing, or an irregular thumping. Some patients, however, have no symptoms at all, and AF is discovered only on a routine ECG or when a stroke occurs — making proactive screening important in those with risk factors.
Classification
The Three Types of AF
AF is classified by how it behaves over time. Understanding the type helps determine both the urgency of treatment and the likelihood of restoring a normal rhythm.
Paroxysmal AF
Episodes that start and stop on their own
Episodes terminate spontaneously, usually within 48 hours but by definition within 7 days. Patients may have frequent episodes or very infrequent ones. Paroxysmal AF still carries a stroke risk and warrants anticoagulation assessment. Rhythm-control strategies to reduce burden are most effective early in the disease course.
Persistent AF
Continuous AF lasting more than 7 days
AF does not self-terminate and requires medical intervention — either cardioversion (electrical reset of the heart) or medication — to restore normal rhythm. The longer AF is present, the more the atria remodel, making rhythm restoration progressively less successful.
Permanent AF
When restoring normal rhythm is no longer possible or pursued
The decision to accept permanent AF focuses management on controlling the heart rate, preventing stroke with anticoagulation, and managing symptoms. Anticoagulation remains essential throughout.
The Most Serious Complication
AF & Stroke Risk
During atrial fibrillation, the atria lose their coordinated contraction. Blood pools and stagnates in the left atrial appendage — a small pouch off the upper chamber — allowing clots to form. These clots can then travel to the brain, causing a potentially devastating and often permanent stroke.
AF-related strokes tend to be severe, as large clots can block major cerebral arteries. The CHA₂DS₂-VASc scoring system quantifies stroke risk by accounting for the patient's age, sex, and other cardiovascular conditions. Patients scoring 2 or above are typically recommended anticoagulation therapy.
Modern DOACs (Direct Oral Anticoagulants) such as apixaban, rivaroxaban, and edoxaban have largely replaced warfarin. They are highly effective, require no regular blood monitoring, and have a better safety profile for most patients.
CHA₂DS₂-VASc Score Factors
- CCongestive heart failure1 pt
- HHypertension1 pt
- A₂Age 75 or over2 pts
- DDiabetes mellitus1 pt
- S₂Prior stroke or TIA2 pts
- VVascular disease (heart attack, PAD)1 pt
- AAge 65–741 pt
- ScSex category (female)1 pt
Score of 2 or above in men (3 or above in women) — anticoagulation is recommended. Dr Nijjer will calculate your score and explain what it means for you.
Investigation
Tests for Atrial Fibrillation
AF may be present on a standard ECG, or it may be paroxysmal and require prolonged monitoring to capture. Structural assessment of the heart is always necessary.
- ECGAn irregular rhythm with absent P-waves confirms AF when present during the recording. If AF is paroxysmal, the resting ECG may be normal.
- Holter Monitor24–48 hour or longer ambulatory ECG monitoring to capture paroxysmal episodes and quantify AF burden over time.
- EchocardiogramAssesses heart structure, valve function, atrial size, and pumping function — all relevant to both cause and treatment planning.
- Blood TestsThyroid function (hyperthyroidism drives AF), kidney function (affects anticoagulant dosing), electrolytes, and full blood count.
- ElectrophysiologyFor selected patients being considered for ablation, detailed mapping of the heart's electrical system guides the procedure.

Management Options
Treating Atrial Fibrillation
AF management has three pillars: preventing stroke, controlling symptoms by managing rate or rhythm, and addressing any underlying causes. Dr Nijjer tailors the strategy to each patient's type of AF, symptoms, and overall health.
Anticoagulation
The single most important intervention for most AF patients. DOACs (apixaban, rivaroxaban, edoxaban) are preferred over warfarin for most patients due to their reliability, safety, and freedom from frequent blood tests.
Rate-Controlling Medications
When AF is accepted, controlling the resting and exercise heart rate to comfortable levels reduces symptoms and protects the heart muscle from rate-related weakening.
- Beta-blockers (bisoprolol, carvedilol)
- Rate-limiting calcium channel blockers
- Digoxin (in selected patients)
DC Cardioversion
A brief controlled electrical shock under sedation resets the heart to normal rhythm. Most effective when performed early. Anticoagulation is required for several weeks before and after the procedure.
AF Ablation
A catheter procedure targeting the electrical triggers of AF — typically around the pulmonary veins in the left atrium. Targeted burns (radiofrequency) or freezing (cryo-ablation) isolate the triggers. Most effective for paroxysmal AF in younger, earlier-disease patients.
Related Conditions
Further Reading
Patient Questions
Atrial Fibrillation FAQs
The questions Dr Nijjer is asked most often about atrial fibrillation — with emergency guidance, his clinical perspective, and trusted external resources.
Medically reviewed by Dr Sukhjinder Nijjer, Consultant Cardiologist (GMC 6103417) · Last reviewed May 2026.
- Chest pain or pressure with the irregular heartbeat
- Severe breathlessness at rest
- Fainting or collapse
- Stroke symptoms — FAST: Face droop, Arm weakness, Speech difficulty → Time to call 999
A first episode that has resolved on its own is not a 999 emergency, but should be assessed in a same-week cardiology clinic.
Jump to a question
- What is atrial fibrillation in simple terms?
- How does AFib cause a stroke?
- Can AFib go away on its own?
- Why do I need anticoagulants for AFib?
- Paroxysmal, persistent and permanent AFib — what is the difference?
- Can I exercise with atrial fibrillation?
- What triggers AFib episodes?
- Medication or ablation — which is better?
- How is AFib diagnosed if my episodes are intermittent?
- Does alcohol cause atrial fibrillation?
What is atrial fibrillation in simple terms?
Atrial fibrillation is a heart rhythm disorder in which the upper chambers of the heart (the atria) quiver chaotically instead of contracting in a coordinated way. The lower chambers respond unpredictably, producing an irregular and often fast pulse that patients often describe as a "fluttering", "racing" or "irregular" heartbeat.
The chaotic atrial activity has two consequences: a less efficient heartbeat (reducing exercise tolerance by around 20–30%), and stagnant blood in pockets of the atrium where clots can form. If a clot is dislodged it can travel to the brain and cause a stroke. AFib is rarely directly life-threatening, but stroke prevention is the most important treatment goal.
How does AFib cause a stroke?
In AFib, the upper heart chambers don't squeeze properly, so blood pools — particularly in a small pouch called the left atrial appendage. Stagnant blood forms clots, and if a clot breaks loose it travels in the bloodstream to the brain, blocks an artery and causes a stroke.
Strokes from AFib are typically larger and more disabling than other strokes because the clots are bigger. People with untreated AFib have around five times the stroke risk of those without — but with appropriate anticoagulation, that risk falls by approximately two-thirds, which is why anticoagulation is the cornerstone of AFib management.
"AFib is one of those conditions where the treatment we have — anticoagulation — is transformatively effective. A well-managed AFib patient on the right anticoagulant has a stroke risk barely above the background population rate. Getting the stroke-prevention decision right matters far more than anything else in AFib management."
— Dr Sukhjinder Nijjer, Consultant Cardiologist
Can AFib go away on its own?
Yes — episodes of paroxysmal AFib can stop spontaneously within minutes, hours or days, and an early first episode can sometimes never come back if a clear trigger (such as a binge drink, an infection or thyroid problem) is identified and removed.
However, if AFib has occurred once, it is more likely to occur again — and over time many patients progress from paroxysmal to persistent or permanent forms. Even when the rhythm self-resolves, the stroke risk while in AFib remains, which is why anticoagulation decisions are based on overall risk profile (CHA₂DS₂-VASc score), not just whether you are currently in AFib.
Why do I need anticoagulants for AFib?
Anticoagulants ("blood thinners") reduce the risk of stroke in AFib by around two-thirds — one of the largest treatment effects in cardiovascular medicine. The decision to start one is based on the CHA₂DS₂-VASc score, which takes into account age, sex, blood pressure, diabetes, heart failure, vascular disease and previous stroke.
Modern direct oral anticoagulants (DOACs — apixaban, rivaroxaban, edoxaban, dabigatran) have largely replaced warfarin in UK practice. They require no blood-test monitoring, have fewer drug interactions, and carry a lower risk of brain bleeds. Aspirin is not an adequate substitute and is no longer recommended for stroke prevention in AFib.
The transformation in AFib stroke prevention over the last decade has been remarkable. Modern direct oral anticoagulants — apixaban, rivaroxaban, edoxaban, dabigatran — are fixed-dose tablets requiring no regular blood test monitoring, and they perform at least as well as warfarin. For most patients with a CHA₂DS₂-VASc score of 2 or more, the benefit of anticoagulation vastly outweighs the small bleeding risk.
The critical message I emphasise to every patient is that missing doses undermines the entire protection. The benefit comes from consistent daily anticoagulation — not occasional treatment. For patients with paroxysmal AFib who ask whether they should take their anticoagulant only when in AFib, the answer is no: stroke risk persists even between episodes. For diagnosis of intermittent episodes, I use ambulatory ECG monitoring and where needed an implantable loop recorder — devices that can record for up to three years.
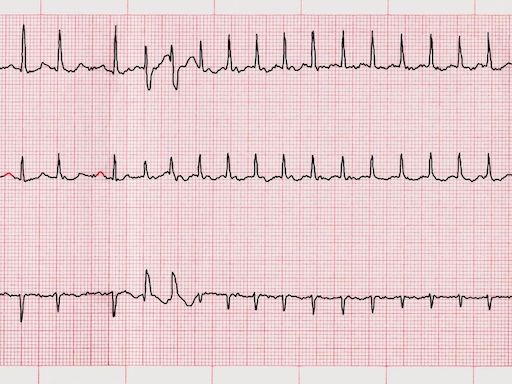
Normal heart rhythm vs atrial fibrillation
Normal sinus rhythm
Regular, evenly-spaced beats arising from the sinus node — the heart's natural pacemaker. Rate 60–100 bpm at rest. Each beat follows a predictable P-wave and QRS complex pattern on ECG.
Atrial fibrillation
Chaotic, irregular rhythm with no organised P-waves. The atria quiver at 350–600 impulses per minute; only some conduct to the ventricles, producing an irregularly irregular pulse. Clot risk from stagnant blood in left atrial appendage.
Paroxysmal, persistent and permanent AFib — what is the difference?
Paroxysmal AFib comes and goes, with episodes lasting less than 7 days and stopping spontaneously. Persistent AFib lasts more than 7 days and usually requires medication or an electrical shock (cardioversion) to restore normal rhythm. Permanent AFib is AFib accepted as the baseline rhythm, with treatment focused on rate control and stroke prevention rather than rhythm correction.
The categories are clinically useful but the boundaries blur — many patients progress through them over time. Stroke risk is similar across all three categories, which is why anticoagulation decisions don't depend on the AFib subtype.
"The patients who do best with AFib are those who understand what their condition is, why they're on anticoagulation, and what their triggers are. Taking 10 minutes in consultation to explain the mechanism properly — the clot forming in that left atrial appendage — makes the difference between someone who takes their DOAC every day and someone who stops it after six months because they feel well."
— Dr Sukhjinder Nijjer, Consultant Cardiologist
Can I exercise with atrial fibrillation?
Yes — for most patients with well-controlled AFib, regular moderate exercise is encouraged and improves both symptoms and long-term outcomes. The exception is very intense endurance exercise, which can both trigger AFib episodes in susceptible people and accelerate the underlying heart remodelling that causes AFib in some athletes.
A sensible target is 150 minutes a week of moderate-intensity activity — walking, swimming, cycling, gardening — plus two sessions of resistance work. If your heart rate climbs unusually high during exercise on AFib, your medication may need adjusting. Speak to your cardiologist before significantly scaling back activity.
What triggers AFib episodes?
Common triggers include alcohol (especially binges — "holiday heart"), poor sleep, dehydration, stress, large meals, caffeine in susceptible individuals, and high-intensity exercise. Sleep apnoea is a particularly important and under-recognised trigger that is frequently missed.
Medical triggers include thyroid overactivity, electrolyte abnormalities, infections, post-surgical states and severe respiratory illness. Keeping a brief diary of episodes and likely triggers is one of the most useful things a patient can do — it often reveals patterns that genuinely change how the condition is managed.
Medication or ablation — which is the better treatment?
Rate-control medication (typically a beta-blocker) is the first step for most patients with mild or well-tolerated AFib. Rhythm-control strategies — antiarrhythmic drugs or catheter ablation — are preferred for symptomatic patients, those with heart failure due to AFib, and increasingly for younger patients with paroxysmal AFib where ablation gives excellent long-term results.
Modern catheter ablation for paroxysmal AFib has a success rate of around 70–80% with one procedure and is now considered first-line therapy for many patients. Anticoagulation continues based on stroke risk regardless of which rhythm strategy is chosen — successful ablation does not by itself permit stopping anticoagulants in most patients.
How is AFib diagnosed if my episodes are intermittent?
Intermittent AFib is diagnosed by capturing an ECG during an episode. Tools include a 24-hour Holter monitor for daily symptoms, a 7-day patch monitor for less frequent episodes, and an implantable loop recorder — a small device under the skin that can monitor for up to three years — for rare but important episodes.
Modern smartwatches (Apple Watch, Fitbit, Withings ScanWatch) with built-in ECG capability are increasingly useful and can produce diagnostic-quality tracings. If you have unexplained palpitations or have had a stroke without an obvious cause, prolonged rhythm monitoring is strongly worth considering.
Does alcohol cause atrial fibrillation?
Yes — alcohol is one of the strongest modifiable risk factors for AFib. A binge of any amount can provoke an episode in susceptible people ("holiday heart"), and regular drinking of more than around 14 units a week roughly doubles the risk of developing chronic AFib.
Importantly, reducing alcohol intake reduces AFib episodes. A randomised trial showed that cutting alcohol from 17 to 2 units a week roughly halved AFib recurrence in symptomatic patients. For anyone with AFib, reducing or stopping alcohol is one of the highest-yield lifestyle interventions available.
Related conditions and investigations
Diagnosed with atrial fibrillation?
Dr Nijjer offers expert AF assessment and management at 68 Harley Street — including stroke risk assessment, rate and rhythm control planning, cardioversion, and referral for ablation where appropriate.