Non-Invasive Cardiac Imaging
CT Coronary Angiography
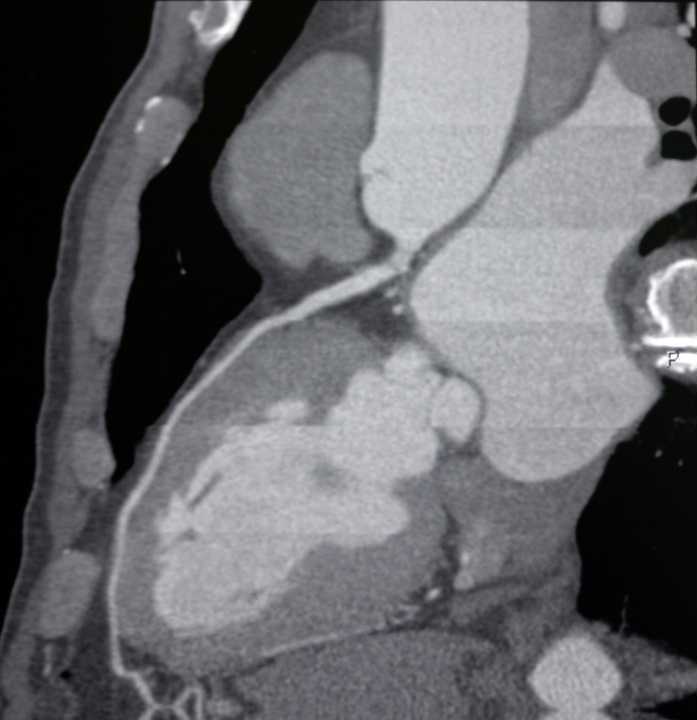
A non-invasive CT scan producing detailed three-dimensional images of the coronary arteries — the most accurate way to rule out significant coronary artery disease without a catheter or hospital admission.

Advanced Non-Invasive Imaging
What Is CT Coronary Angiography?
CT coronary angiography (CTCA) uses a modern multi-slice CT scanner and iodine-based contrast dye to produce detailed, high-resolution three-dimensional images of the coronary arteries and the plaque within them. The result is a comprehensive map of the coronary anatomy, obtained without the need for a catheter, arterial puncture, or hospital admission.
CTCA has transformed the assessment of chest pain. The NICE guidelines now recommend it as the first-line investigation for patients presenting with new chest pain at low-to-intermediate risk of obstructive coronary artery disease. Its outstanding negative predictive value — above 99% — means a normal CTCA effectively excludes significant coronary disease with very high confidence.
Importantly, CTCA detects both obstructive plaques (those narrowing the artery lumen) and non-obstructive plaques (those causing some thickening of the arterial wall without yet causing significant narrowing). Identifying non-obstructive disease allows targeted preventative treatment — statins, aspirin, and lifestyle modification — before any heart attack or angina develops.
Dr Nijjer reviews every CTCA result in collaboration with specialist cardiothoracic radiologists, and discusses the findings with you in detail at your follow-up appointment.
Atherosclerosis Burden
The Coronary Artery Calcium Score
Quantifying Coronary Calcification
A calcium score (Agatston score) is often performed as part of the CTCA protocol — or sometimes as a separate, very low radiation scan before contrast is given. Coronary artery calcification is a direct marker of atherosclerotic plaque burden in the artery wall. Even without any symptoms or risk factors, a high calcium score identifies individuals at significantly elevated cardiovascular risk.
A score of zero is profoundly reassuring — in the absence of symptoms, it is associated with a very low 10-year cardiovascular event rate and may allow deferral of preventative medications. Scores above 400 indicate heavy calcification and mandate aggressive risk factor modification.
- 0No calcification — very low risk
- 1–100Mild — low risk
- 101–400Moderate — intermediate risk
- >400Severe — high risk
What to Expect
The Scan Procedure
Preparation
A cannula is placed in your arm vein. ECG electrodes monitor your heart rate. Women of childbearing age (under 55) are asked about pregnancy before proceeding. A beta-blocker tablet or injection may be given to slow the heart rate to around 60 bpm for sharper images.
Positioning
You lie on your back on the CT scanner table with your arms raised above your head. You are moved through the circular CT gantry while the team operates the scanner from an adjacent room with a clear window, remaining in communication with you throughout.
Contrast Injection
Iodine-based contrast dye is injected rapidly through your cannula. You may experience a warm flushing sensation throughout the body and a metallic taste in the mouth — both are normal, harmless, and pass within seconds.
The Scan
You are asked to hold your breath for approximately 10–15 seconds while the CT acquires images. The actual scanning time is very short. A second breath-hold sequence may be needed. The entire procedure from arrival to departure typically takes 60–90 minutes.
Recovery & Results
You may eat and drink normally after the scan. Drink extra water to help flush the contrast. Blood pressure is monitored briefly if a beta-blocker was given. Results are reviewed by Dr Nijjer with specialist radiologists, then discussed at a follow-up consultation.
Understanding Your Findings
What Happens After Your Scan
The CTCA result determines the next clinical step. Dr Nijjer will explain which pathway applies to you and what it means for your treatment plan. Most results fall into one of three categories.
Result 1 — Reassuring
Normal or Near-Normal Arteries
The coronary arteries appear entirely normal, or show only minimal non-obstructive plaque with no haemodynamically significant narrowing. This is a highly reassuring finding with a very low risk of future cardiac events.
In most patients this result effectively excludes angina as the cause of symptoms and allows Dr Nijjer to pursue alternative diagnoses or focus on cardiovascular risk reduction with lifestyle and preventative medications.
Result 2 — Intermediate
Non-Obstructive Coronary Disease
Plaques are visible within the coronary artery walls but do not significantly narrow the lumen. These plaques do not cause angina at this stage but represent established atherosclerosis and an elevated future risk of heart attack.
Functional testing — stress echocardiography or stress perfusion cardiac MRI — may be performed to determine whether any haemodynamic impact is present. Medical treatment with statins, antiplatelet agents, and lifestyle measures is recommended.
Result 3 — Significant
Obstructive Coronary Artery Disease
One or more coronary arteries show significant narrowing (>50–70% stenosis) that is likely to be limiting blood supply to the heart muscle. This finding requires further evaluation to determine whether intervention is needed.
Invasive coronary angiography is typically the next step, allowing precise physiological assessment with iFR or FFR pressure wire measurement and, if appropriate, coronary angioplasty and stenting in the same procedure.
Safety Information
Risks & Considerations
Radiation Exposure
CTCA involves ionising radiation. Modern scanners with dose-reduction algorithms typically deliver an effective dose of 1–3 mSv — comparable to 6–15 months of natural background radiation in the UK. The clinical benefit of the information obtained vastly outweighs this small risk for appropriately selected patients. CTCA is not recommended in pregnancy.
Contrast Reactions
Iodine contrast dye can occasionally cause an allergic-type reaction. Mild reactions (flushing, nausea, urticaria) occur in approximately 1–3% of patients. Severe anaphylactic reactions are very rare (<0.04%). A team trained in managing contrast reactions is present during every scan, with medications immediately available.
Kidney Function
Iodine contrast is cleared through the kidneys. Patients with significantly impaired renal function (eGFR below 30 mL/min/1.73m²) are at risk of contrast-induced nephropathy. Alternative investigations — stress perfusion cardiac MRI using gadolinium, or nuclear perfusion imaging — are used instead. Kidney function is checked before every CTCA if there is any concern.
Concerned About Your Coronary Arteries?
CT coronary angiography provides a definitive, non-invasive answer. Dr Nijjer selects, arranges, and personally reviews every scan for his patients.