Procedure — Cardiac Electrophysiology
Cardiac
Pacemakers
A pacemaker is a small device implanted below the collarbone to treat dangerously slow heart rates and pauses. Modern pacemakers are reliable, long-lasting, and allow patients to return quickly to a full and active life.

Device Overview
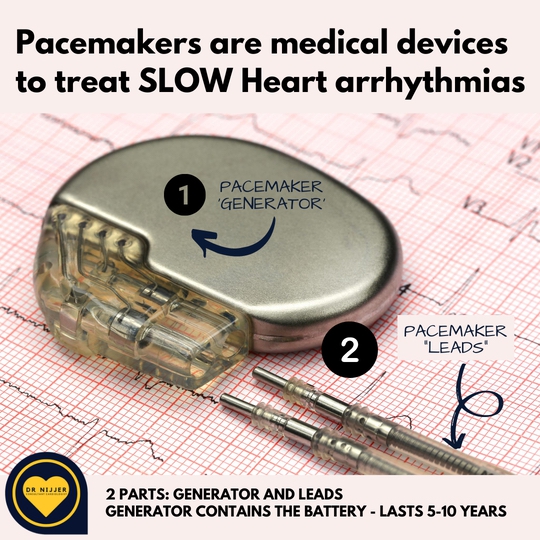
What Is a Pacemaker?
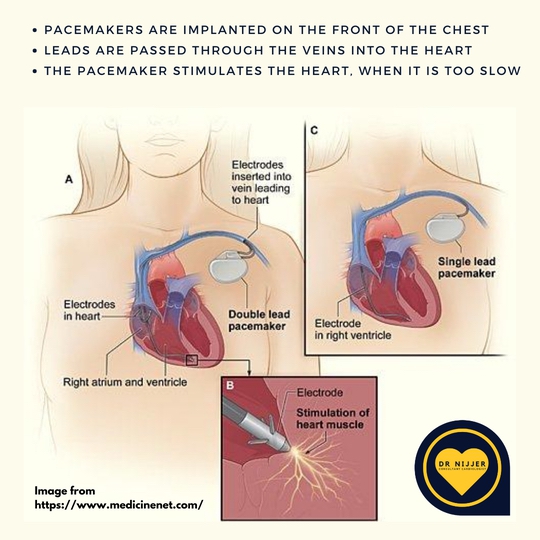
A pacemaker is a small medical device — typically smaller than a pack of matches — implanted beneath the skin just below the collarbone. It is connected to one or two leads (wires) that travel through a vein into the right side of the heart.
The device continuously monitors the heart's electrical activity. When it detects that the heart rate has dropped too low, or that a pause has occurred, it delivers a small electrical impulse to stimulate the heart muscle to contract — maintaining a safe minimum heart rate.
Most modern devices are dual-chamber pacemakers, with leads in both the right atrium and right ventricle. This allows coordinated pacing that mimics the natural sequence of the heartbeat, preserving the atrial contribution to cardiac output. Single-chamber devices may be used in patients with permanent atrial fibrillation or in frail elderly patients where simplicity is preferred.


When It Is Required
When Is a Pacemaker Needed?
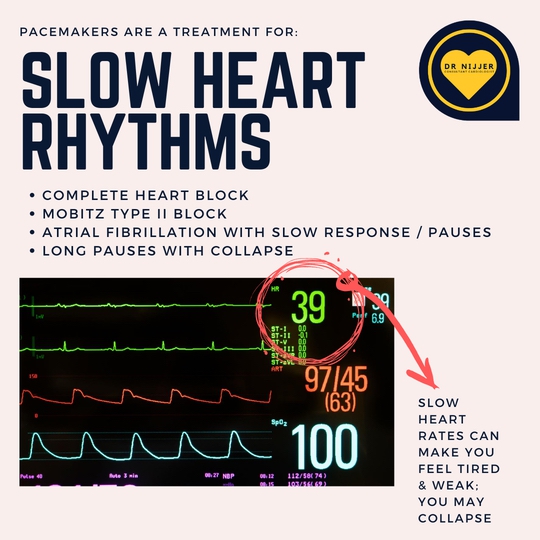
Pacemakers are implanted when the heart's natural electrical system fails to maintain an adequate rate — producing symptoms of dizziness, blackouts, or near-fainting. The decision is based on symptoms, the length of pauses, and the type of electrical abnormality.
Symptomatic Bradycardia
A resting heart rate that is consistently too slow — particularly when accompanied by dizziness, fatigue, or exertional limitation. Pauses exceeding 3 seconds with symptoms typically warrant pacemaker consideration.
Complete Heart Block
The electrical connection between the atria and ventricles is disrupted, so the lower chambers beat independently at a dangerously slow rate. This is an urgent indication that may require emergency implantation.
Significant Pauses
Nighttime pauses of 6 seconds or longer are generally considered an indication for pacing, even without daytime symptoms. Prolonged pauses can cause loss of consciousness and risk a fall or injury.
Sick Sinus Syndrome
The sino-atrial node — the heart's natural pacemaker — fails to generate reliable, regular impulses, causing unpredictable alternation between very slow and occasionally fast rates.
AF with Slow Rate
Atrial fibrillation with a slow ventricular response, particularly when rate-controlling medications must be used that would otherwise be unsafe without pacing support.
Post-Heart Attack
Damage to the heart's conduction system during a heart attack, particularly from right coronary artery occlusion, can require temporary or permanent pacing.
Step by Step
The Implantation Procedure
The procedure is performed under local anaesthetic with light sedation — patients are awake but comfortable throughout. It typically takes 60–90 minutes and most patients go home the following day.
Preparation
Blood tests, antibiotic prophylaxis. Most antiplatelet medications (aspirin, clopidogrel) are continued. Anticoagulants may need a short pause.
Local Anaesthetic
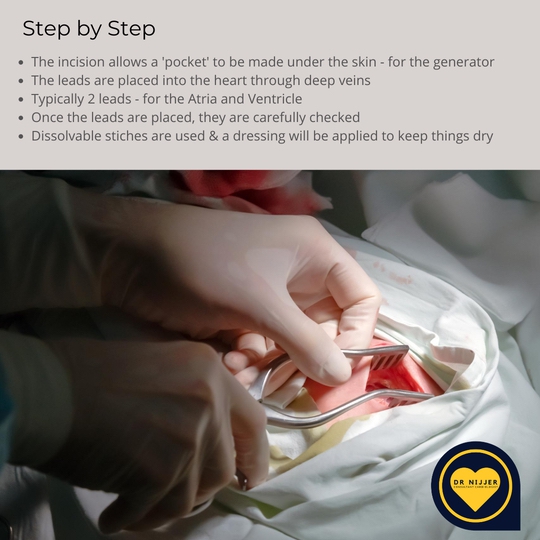
A local anaesthetic is injected below the collarbone. Light intravenous sedation keeps the patient comfortable. A 3–4 cm incision is made.
Lead Placement
Leads are guided through the subclavian vein into the heart under continuous X-ray (fluoroscopy) guidance, and positioned precisely for optimal sensing and pacing.
Device Testing
Pacing thresholds, sensing, and lead stability are verified before the device generator is connected and placed in a pocket beneath the skin.
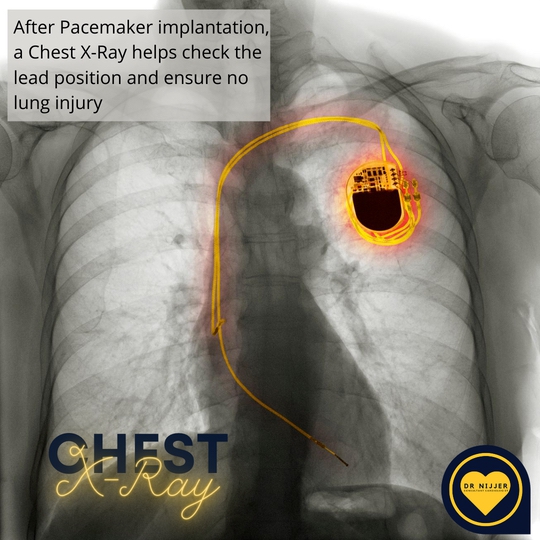
Closure & X-Ray
The wound is closed and a chest X-ray confirms correct lead position and excludes pneumothorax. Pacemaker checks follow over the subsequent days and weeks.
After the Procedure
Recovery & Post-Operative Care
The first six weeks are the most critical period. Following these guidelines protects the leads while they bed into the heart wall.
- Restrict the arm on the implant side (usually the left) for 6 weeks — treat it as though it is broken. Do not raise it above shoulder height.
- No overhead activity — gardening, swimming, racquet sports, and lifting are restricted until Dr Nijjer confirms lead stability.
- Wound care — keep the incision clean and dry. Bruising and some swelling over the device pocket is normal in the first 1–2 weeks.
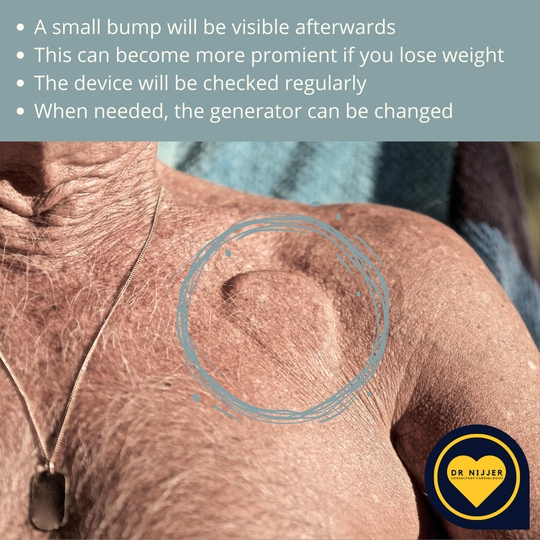
- Device checks — the pacemaker is checked before discharge, again in 4–6 weeks, then at 6 months, then annually thereafter.
- Do not manipulate the device — the pacemaker may be visible as a small bulge. Pressing on it or moving it could retract the leads.
- Driving — DVLA guidelines apply. In the UK, most patients can return to driving after 1 week (private licence) if the device was implanted prophylactically. Dr Nijjer will advise based on the indication.

Risks & Complications
Potential Complications
Pacemaker implantation is a routine procedure with an excellent safety record. As with all surgical procedures, complications can occur, though serious events are uncommon. Dr Nijjer will discuss the specific risks relevant to each patient beforehand.
Bruising & Haematoma
Bleeding at the incision site or into the device pocket. Usually resolves spontaneously; occasionally requires drainage.
Wound Infection
Superficial infections are treated with antibiotics. Deep device infection is rare but serious, potentially requiring device removal and prolonged antibiotic treatment.
Pneumothorax
Accidental puncture of the lung during venous access can cause the lung to collapse. Detected by the post-procedure chest X-ray; most resolve without intervention.
Lead Displacement
Rarely, a lead moves from its original position before it has fully embedded. This may require a return to the procedure room to reposition it — most common in the first 6 weeks.

After Six Weeks
Long-Term Living with a Pacemaker
Once the leads have settled and function has been confirmed, most patients return to full normal activities. The device does not limit daily life — the majority of patients are simply unaware of it.
Battery life varies with pacing demand but typically lasts 8–12 years. When the battery nears depletion, the generator is replaced under local anaesthetic; the leads remain in place and are reused. This is a shorter, simpler procedure than the original implantation.
The device may be prominent under the skin in thinner individuals. Patients should avoid pressing or manipulating it. Significant weight loss may increase prominence; in rare cases of very thin overlying skin, revision of the pocket position may be considered.
Everyday electrical devices — mobile phones, microwave ovens, airport security scanners — do not affect modern pacemakers. Patients should carry their device identification card and inform medical teams before procedures involving strong magnetic fields (some MRI protocols) or surgical diathermy.
Pacemaker-Friendly MRI
Most modern pacemakers are MRI-conditional — compatible with MRI scans under specific conditions. Dr Nijjer uses MRI-conditional devices where appropriate, preserving full diagnostic imaging access for the future.
Follow-Up Schedule
- Before dischargePacemaker interrogation to confirm correct settings
- 4–6 weeksWound review and lead stability check
- 6 monthsFull device check and pacing threshold optimisation
- AnnuallyRoutine device clinic to assess battery status and function
Related Conditions
Further Reading
Referred for a pacemaker?
Dr Nijjer implants pacemakers as part of his NHS practice and offers private consultation at 68 Harley Street to discuss whether a pacemaker is the right treatment for you, what to expect from the procedure, and how to manage life with a device.