Coronary Artery Disease
Coronary Heart
Disease
The UK's leading cause of death — yet with expert assessment and timely treatment its progression can be slowed, halted, and in many cases reversed.

Overview
What is Coronary Heart Disease?
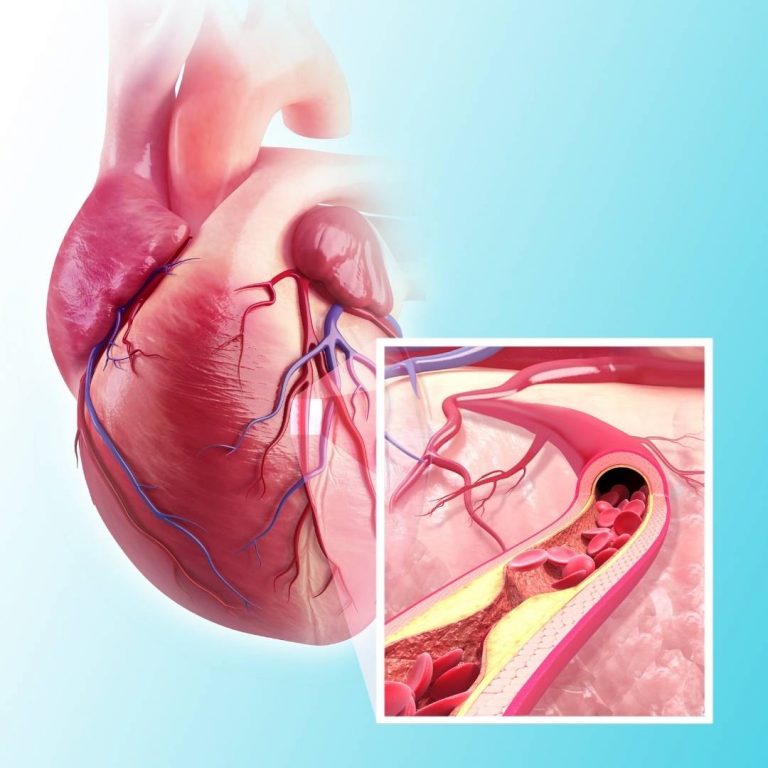
Coronary heart disease is a condition in which a fatty substance — called atheroma or plaque — builds up within the arteries that supply blood to your heart. As this atheroma accumulates, it deprives the heart muscle of the oxygen and nutrients it needs.
The consequences depend on how quickly the disease progresses. A slow, gradual build-up typically causes angina — chest tightness on exertion. A sudden rupture of the plaque triggers blood clotting, which can block the artery entirely and cause a heart attack. Long-standing disease can also weaken the heart muscle and lead to heart failure.
This page covers the anatomy of the coronary arteries, the process of atherosclerosis, the 12 recognised risk factors, common symptoms, the tests used to diagnose CHD, and the treatments available.
Anatomy
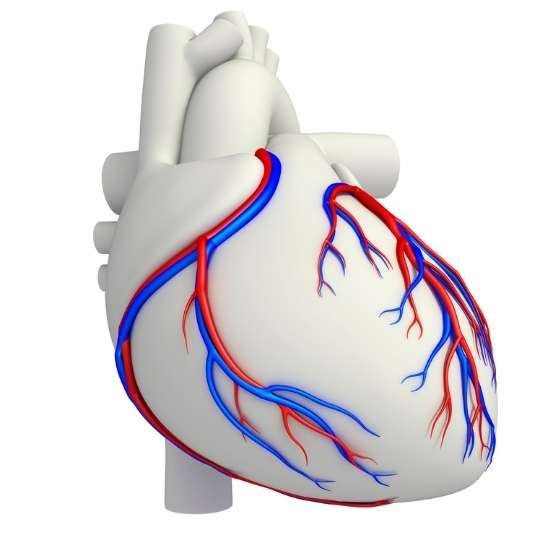
The Heart and its Arteries
The heart is a pump made of specialised muscle that must nourish itself through its own network of arteries — known as the coronary arteries.
There are two principal coronary arteries, but the left coronary artery divides almost immediately into two branches. In practice, we refer to three main vessels:
- Left Anterior Descending (LAD) — supplies the front of the heart
- Left Circumflex Artery (LCx) — supplies the back and left side
- Right Coronary Artery (RCA) — supplies the right side and inferior heart
The origin of the left coronary artery — called the Left Main Stem (LMS) — is a critical structure. Disease at this location supplies jeopardy to the majority of the heart muscle and requires specialist additional treatments.
The coronary arteries begin at around 4–5 mm in diameter and taper as they travel through the heart muscle. Beyond the visible vessels lies the microcirculation — tiny vessels invisible to conventional imaging but responsible for the final delivery of blood to the heart muscle cells.
If there is a problem with one of the coronary arteries, all the heart muscle supplied by that vessel is at risk of damage or death.
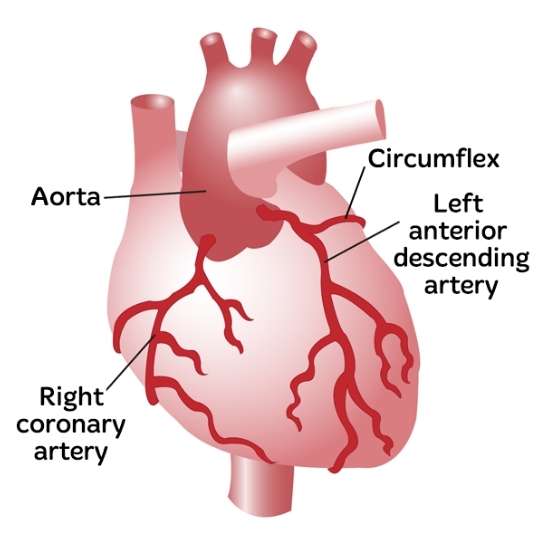
The three main coronary arteries and the Left Main Stem
How It Develops
Atherosclerosis — The Process of Plaque Build-Up
Stage One
Artery Injury
The smooth artery lining is damaged by factors such as smoking, high blood pressure, or diabetes. Inflammatory cells begin to infiltrate the vessel wall.
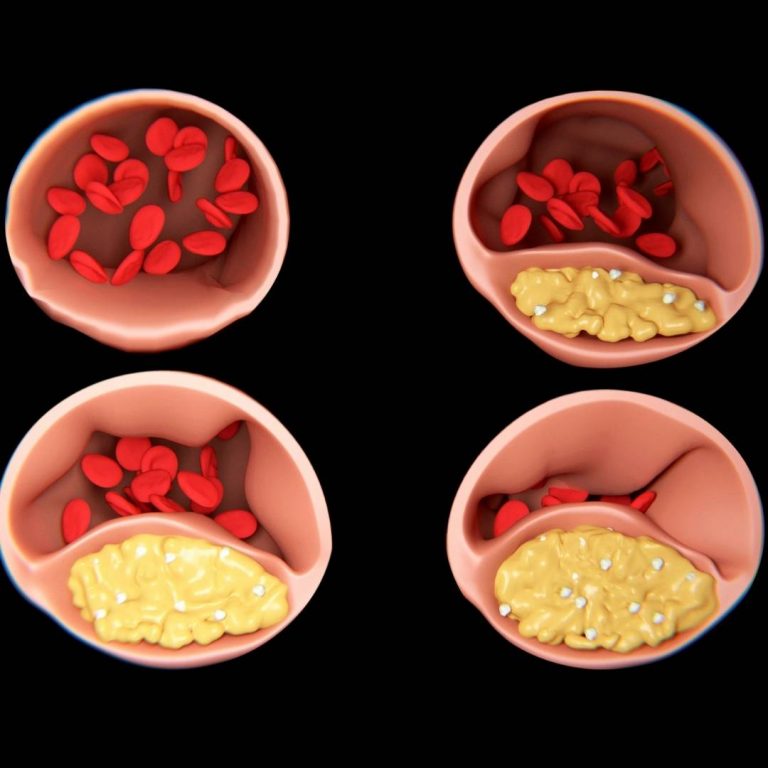
Stage Two
Plaque Build-Up
Cholesterol and fatty substances adhere to the injured wall. Layers of cholesterol-laden cells accumulate, progressively narrowing the artery lumen and restricting blood flow.
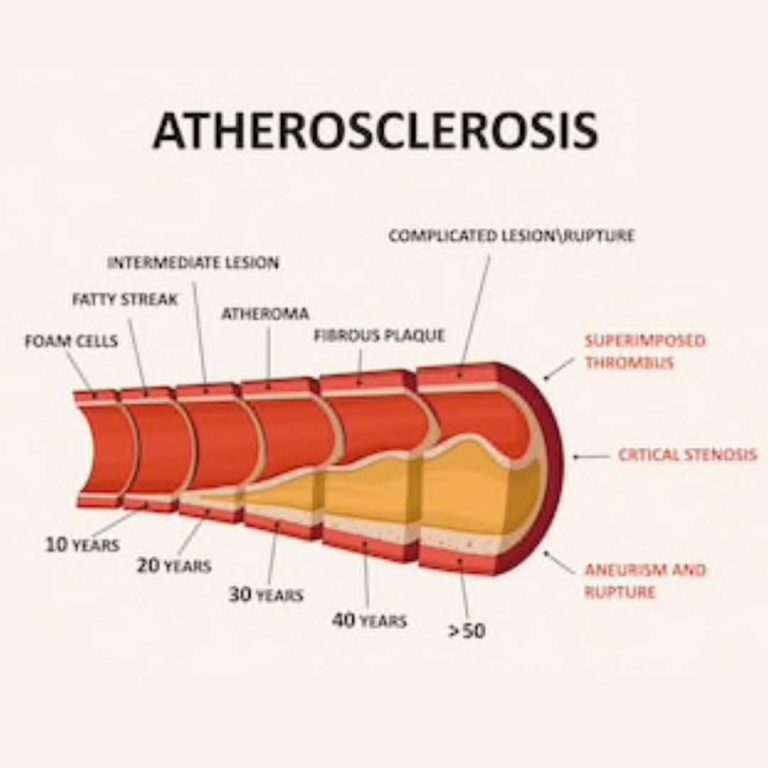
Stage Three
Rupture & Clot
An unstable plaque can rupture suddenly. Blood clots rapidly on the exposed material and, because coronary arteries are small, even a tiny clot can block the vessel entirely — causing a heart attack.
The build-up of atherosclerosis is often compared to domestic pipes clogging with debris. When the lumen narrows significantly, the heart muscle supplied by that artery receives insufficient blood during exertion. At rest the supply may be adequate, but when the heart rate rises during physical activity, blood flow becomes insufficient and symptoms of angina develop.
When a plaque ruptures suddenly, the collagen and cholesterol material exposed to flowing blood triggers immediate clot formation. Because coronary arteries are small, even a modest clot can occlude the vessel completely. This is a heart attack — and opening the artery as quickly as possible using angioplasty is essential to limit damage to the heart muscle.
Risk Factors
What Increases the Risk of Coronary Heart Disease?
There are 12 recognised risk factors for coronary heart disease. Four are fixed and cannot be changed — but understanding them helps determine how aggressively you should manage the eight risk factors that you can improve.
Factors You Cannot Control
01
Age
Coronary heart disease increases with age as it is a slow and progressive condition. Older patients are more likely to have severe, heavily calcified blockages that can be difficult to treat with standard techniques. Dr Nijjer is trained in complex calcium modification including rotational atherectomy and shockwave balloons for this group.
02
Gender
Men are more likely to develop coronary heart disease at a younger age. After the menopause, however, a woman's risk rises sharply to approach that of men. Women often present to doctors later and are statistically less likely to be offered testing — Dr Nijjer is committed to equal assessment regardless of gender.

03
Ethnicity
People with a South Asian background (Indian, Pakistani, Bangladeshi, Sri Lankan) have significantly higher rates of coronary artery disease. Those of African or Afro-Caribbean heritage carry a higher risk of hypertension and stroke. Both groups also have elevated rates of Type 2 Diabetes, itself a strong risk factor for coronary disease.

04
Family History
Heart disease is polygenic — many genes each contribute a small risk. If relatives carry genes for high cholesterol, high blood pressure, or altered cholesterol metabolism, your risk can be substantially elevated.
You have a strong family history if your father or brother had heart disease under age 55, or your mother or sister under age 65.
An important inherited condition is Familial Hypercholesterolaemia — a defect in cholesterol-receptor genes causing very high cholesterol from childhood. Specialist treatment is essential for this group.
Risk Factors You Can Improve
These four risk factors are the most important targets for treatment. Making progress on even one or two of them significantly reduces your lifetime risk of heart attack.

High Blood Pressure
Hypertension causes no symptoms yet is a major driver of coronary disease worldwide. Elevated pressure acts as a continuous source of injury to the artery lining — directly triggering the atherosclerosis process. It also accelerates damage to the brain's small arteries, raising the risk of stroke. Many patients are in denial and decline treatment — early management is strongly advised.
High Cholesterol
Cholesterol is a fatty substance naturally produced by the liver and essential for many body processes — but excess levels drive atherosclerosis. A full lipid profile measures total cholesterol, HDL ("good" cholesterol), LDL ("bad" cholesterol) and triglycerides. In patients with confirmed coronary disease or prior heart attack, LDL should be reduced as low as possible. Modern cholesterol tests do not require fasting.

Diabetes
Diabetes — particularly Type 2 Diabetes — is rapidly increasing worldwide and dramatically accelerates coronary artery disease when it interacts with high blood pressure and raised cholesterol. Excellent blood sugar control, weight loss, regular exercise, and not smoking are all essential. For those with diabetes, the combination of risk factors is highly atherogenic and requires aggressive management.

Smoking
Smoking increases risk through multiple mechanisms. Carbon monoxide binds to haemoglobin and starves tissues of oxygen. Nicotine causes coronary arteries to constrict and can trigger vasospasm, acutely worsening blood flow around any existing narrowing. Cigarette chemicals directly injure the artery lining and promote bad cholesterol to adhere. The combination of smoking with high blood pressure, high cholesterol, or diabetes is particularly dangerous.
Modern Day Risk Factors
Modern lifestyles have introduced four additional risk factors that have become increasingly significant contributors to coronary artery disease.

Poor Diet
Diets high in fat, salt, sugar, and processed foods increase the risk of coronary heart disease. Making a concerted effort to reduce processed food intake and replace it with fresh vegetables, lean proteins, and healthy fats can meaningfully reduce both cholesterol and blood pressure over time.

Lack of Physical Activity
Modern desk-based work and sedentary leisure time mean many people are significantly under-active. Physical inactivity raises cholesterol, contributes to high blood pressure, and promotes insulin resistance and Type 2 Diabetes.
Regular exercise can reduce your risk of heart disease by around a third.

Air Pollution
London's air contains fine particles from diesel vehicles and other sources — including nitrogen dioxide, sulphur dioxide, and carbon monoxide — that trigger artery injury, alter coronary artery movement, and increase blood clotting tendency. On high-pollution days, exercise indoors or in rural areas where possible. Check levels on the government's UK-AIR website.
Stress
Prolonged work and financial stress chronically elevates blood pressure and promotes poor lifestyle choices — comfort eating, excess alcohol, and reduced physical activity. In the short term, stress is a useful driver of performance. Over the long term, its cardiovascular effects are significant. Regular physical activity, reduced caffeine and alcohol, and mindfulness or meditation practices all help manage its impact.

Recognising CHD
Symptoms of Coronary
Heart Disease
Symptoms depend on the speed of disease progression. A slow build-up causes progressive angina; some patients have no symptoms at all until a heart attack. Common symptoms include:
- Chest tightness, pressure, or pain — often on exertion
- Heaviness or pressure in the arms during activity
- Breathlessness, particularly on exertion
- Palpitations or an irregular heartbeat
- Dizzy spells or blackouts on exertion
- Nausea or an unsettled stomach during activity
Sudden severe chest pressure with pain radiating into the arm, sweating and nausea together may indicate a heart attack. Seek emergency medical attention immediately.
Atherosclerosis can be entirely silent — many patients with severe coronary artery disease have no typical symptoms. Screening and risk assessment are therefore important even in the absence of symptoms.
Assessment
Diagnostic Tests for Coronary Heart Disease
Dr Nijjer will take a thorough personal and family history before recommending the right combination of tests. Bringing any previous blood test results or health screen reports to your appointment can help streamline assessment.

Test 01
Electrocardiogram (ECG)
A rapid, non-invasive snapshot of the heart's electrical signals. Essential baseline information, though a normal ECG does not exclude significant coronary disease.

Test 02
Echocardiogram
An ultrasound examination of the heart that assesses pump function and wall motion. In patients with significant coronary disease, the heart muscle can become weakened and this will be visible on the echo.

Test 03
CT Coronary Angiogram
A non-invasive scan that visualises the coronary arteries and measures the calcium score — a powerful predictor of future heart attack risk — as well as soft plaque and the degree of any narrowing.

Test 04
Invasive Coronary Angiography
The gold standard for diagnosing coronary disease. Performed through the wrist artery, a thin catheter is guided to the coronary arteries, allowing direct visualisation and pressure-wire (iFR) flow measurement within the same procedure.
Management
Treating Coronary
Heart Disease
Treatment is tailored to the severity of your disease, your risk of future events, and your individual circumstances. All patients will be counselled on lifestyle optimisation — but many will also require medication, and some will need a procedure.
Lifestyle & Risk Factor Management
Addressing the modifiable risk factors — blood pressure, cholesterol, diabetes, smoking, diet, activity, and stress — is the foundation of treatment. Even in patients who need medication or a procedure, lifestyle optimisation remains essential.
Medications
- Aspirin 75mg — reduces platelet activity and lowers the risk of clot formation on any existing plaque.
- Statins — highly effective cholesterol-lowering drugs that are safe and have been validated over decades. Patients with confirmed coronary disease or a prior heart attack require higher doses to drive LDL as low as possible.
- Blood pressure medication — targeted agents to reduce arterial pressure and slow the progression of coronary disease.
Coronary Intervention
When narrowings are haemodynamically significant — meaning they are actually restricting blood flow — coronary angioplasty (PCI) is used to open the artery and restore normal flow. Dr Nijjer is an internationally recognised expert in complex angioplasty, including calcium modification with shockwave balloons, rotational atherectomy, and laser treatment for challenging lesions.
Read about Angioplasty →
Coronary angioplasty restores blood flow through narrowed or blocked arteries
Dr Nijjer has developed the iFR pressure-wire technique — now used worldwide to guide which narrowings truly need treatment, avoiding unnecessary interventions.
Further Information
Additional Resources
The British Heart Foundation provides comprehensive patient information on coronary heart disease, including downloadable PDF guides and support resources.
Dr Nijjer's peer-reviewed research on coronary physiology, iFR technology, and complex coronary intervention is available through PubMed.
Related Conditions
You May Also Find Helpful
Concerned About Your
Coronary Arteries?
Dr Nijjer offers same-week appointments at Harley Street and across London. GP referrals and self-referrals are equally welcome.