Symptoms — Cardiac Investigation
Breathlessness &
Shortness of Breath
Breathlessness — medically termed dyspnoea — is a subjective sensation of breathing discomfort. It is one of the most common reasons for cardiology referral and can arise from both cardiac and respiratory causes, many of which are treatable.

Understanding the Symptom
What Is Breathlessness?
Breathlessness is defined as a subjective experience of discomfort during breathing. It is a symptom — not a diagnosis — and the underlying cause must be identified before appropriate treatment can be prescribed.
Presentations vary widely. Some patients feel an inability to take a satisfying breath; others experience shallow rapid breathing, a sensation of air hunger, or a feeling that their chest will not fully expand. The symptom can be acute — developing over hours or days — or chronic, persisting over weeks to months.
As a cardiologist, Dr Nijjer investigates whether the breathlessness arises from a cardiac source — the heart's inability to pump efficiently, abnormal rhythm, or insufficient blood supply — while working alongside respiratory physicians when a lung cause is suspected.

Differential Diagnosis
Cardiac vs Respiratory Causes
Identifying whether the cause is cardiac or respiratory — or a combination of both — is the key first step in investigation. Many patients have contributing factors from both systems.
Investigated by Dr Nijjer
Cardiac Causes
- Heart Failure — the heart cannot pump enough blood to meet the body's demands, causing fluid to back up into the lungs
- Coronary Heart Disease & Ischaemia — insufficient blood supply to the heart muscle during exertion
- Arrhythmias — atrial fibrillation, fast or slow heart rhythms that reduce pumping efficiency
- Valve Disease — narrowed or leaking heart valves that impede normal blood flow
- Pericardial Disease — fluid around the heart compressing the chambers
- Severe Anaemia — insufficient oxygen-carrying capacity reducing cardiac output
Respiratory / Other
Non-Cardiac Causes
- COPD — chronic obstructive pulmonary disease causing progressive airflow limitation
- Asthma — reversible airway narrowing triggered by allergens or irritants
- Pneumonia — lung infection reducing the available surface for gas exchange
- Pulmonary Fibrosis — progressive scarring of lung tissue
- Pleural Effusion — fluid around the lung compressing lung tissue
- Deconditioning — reduced cardiovascular fitness from prolonged inactivity
Onset & Duration
Acute vs Chronic Breathlessness
The speed of onset gives important diagnostic information and helps direct the urgency and type of investigation required.
Acute Breathlessness
Rapid-onset breathlessness — developing within hours — may indicate acute heart failure, a pulmonary embolism (blood clot in the lung), severe asthma, or pneumonia. This warrants prompt hospital assessment, as some causes are life-threatening without rapid treatment.
Chronic Breathlessness
Gradual onset over weeks or months suggests a progressive condition — heart failure, COPD, pulmonary fibrosis, or anaemia. Dr Nijjer investigates these systematically to establish the primary cause before planning treatment.
Investigation
Tests for Breathlessness
A structured set of investigations is used to identify whether the cause is cardiac, respiratory, or a combination of both. Dr Nijjer tailors the sequence to each patient's presentation.
ECG
Identifies arrhythmias, signs of heart muscle damage, or electrical conduction problems that could contribute to breathlessness.
View test →Echocardiogram
Ultrasound of the heart — assesses pumping function, valve appearance, and whether fluid has accumulated around the heart.
View test →Chest X-Ray
Identifies fluid on the lungs, heart enlargement, pneumonia, or lung collapse.
Blood Tests
Checks for anaemia, thyroid disease, BNP (a heart failure marker), and inflammatory markers.
Lung Function Tests
Spirometry measures airflow and identifies obstructive (asthma, COPD) or restrictive (fibrosis) lung patterns.
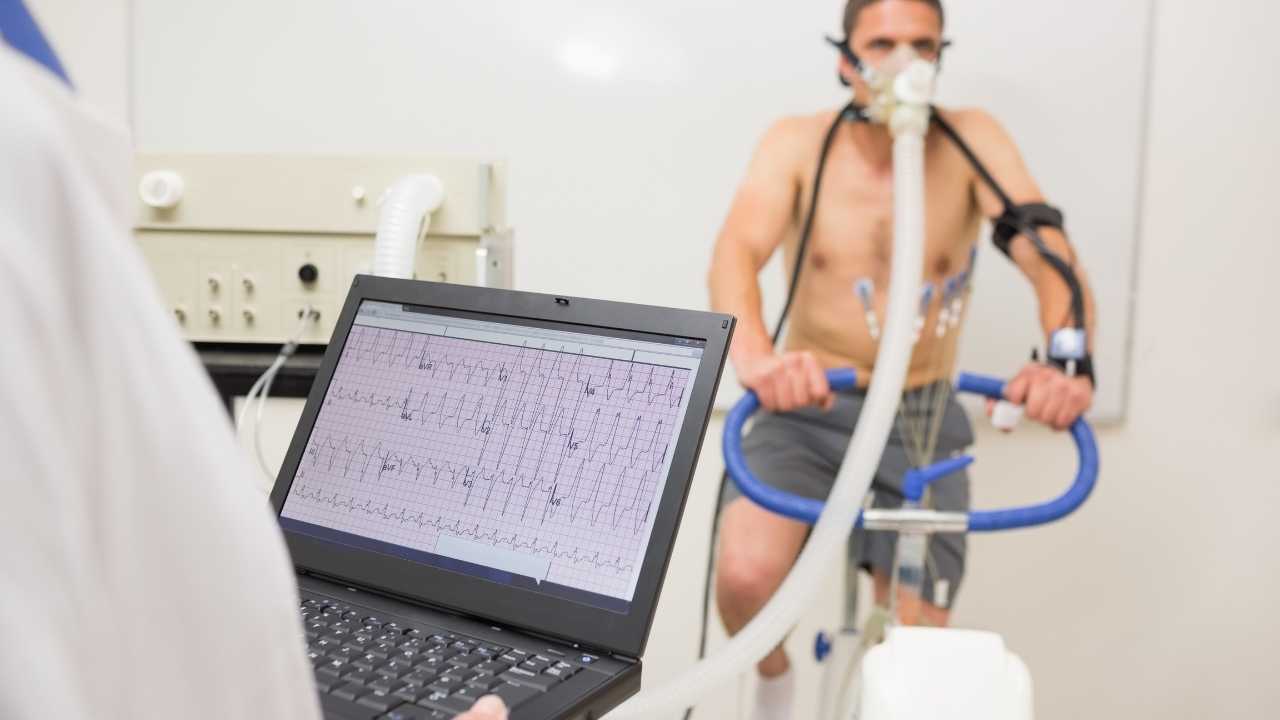
Exercise Stress Testing
Assesses breathlessness that occurs only on exertion and may reveal hidden ischaemia or impaired cardiac reserve.
View test →
Management
Treatment & Management
Treatment is directed entirely at the underlying cause, which is why accurate diagnosis is the essential first step. There is no single treatment for breathlessness — the correct approach depends entirely on whether the cause is cardiac, respiratory, or systemic.
For cardiac causes, this may include heart failure medications, correction of an arrhythmia, valve intervention, or coronary angioplasty to restore blood supply to an ischaemic region of heart muscle.
For respiratory causes, treatment may involve inhalers, steroids, antibiotics, pulmonary rehabilitation, or smoking cessation programmes.
For deconditioning — increasingly common following periods of illness or inactivity — a structured graded exercise programme can produce dramatic improvements in breathlessness and quality of life.
Related Conditions
Further Reading
Patient Questions
Breathlessness & Heart Failure FAQs
The questions Dr Nijjer is asked most often about breathlessness and heart failure — including how to tell cardiac from non-cardiac causes, and what modern treatment can achieve.
Medically reviewed by Dr Sukhjinder Nijjer, Consultant Cardiologist (GMC 6103417) · Last reviewed May 2026.
Heart failure and breathlessness at One Heart Clinic
Breathlessness is one of the most important cardiac symptoms and requires systematic investigation. Dr Nijjer assesses both the severity and the underlying cause — whether cardiac, pulmonary or mixed — and coordinates the right treatment.
- Echocardiogram to assess heart function and valve disease
- Cardiac MRI for detailed myocardial assessment
- BNP and NT-proBNP blood markers for heart failure
- Coordinated management with heart failure specialist teams

Echocardiogram showing heart function — the key test in breathlessness assessment
- Sudden, severe breathlessness at rest
- Breathlessness combined with chest pain or pressure
- Blue lips or fingertips (cyanosis)
- Collapse or near-collapse with breathlessness
These symptoms can indicate pulmonary embolus, acute heart failure or a heart attack. Do not wait — call 999 immediately.
Jump to a question
- Why do I get out of breath walking upstairs?
- Is breathlessness always a heart problem?
- What is heart failure and is it reversible?
- Can heart failure be cured?
- Why are my ankles swollen?
- What is the life expectancy with heart failure?
- Can an irregular heartbeat cause breathlessness?
- What tests diagnose the cause of breathlessness?
- Is it normal to feel breathless after COVID?
- Heart failure vs a weak heart — what is the difference?
Why do I get out of breath walking upstairs?
The single commonest cause of breathlessness on stairs is deconditioning — a fall in cardiovascular fitness from reduced activity. The next commonest are excess weight, anaemia and asthma. In older adults or those with risk factors, early heart failure, coronary disease and valve problems all need to be considered.
A useful distinction: deconditioning usually feels like a generalised tiredness and recovers within a few minutes of stopping. Cardiac breathlessness often comes with a heavier chest sensation, tends to be reproducible at the same level of exertion each time, and may be accompanied by ankle swelling or breathlessness when lying flat. A change in your usual exercise capacity over weeks or months always deserves assessment.
Is breathlessness always a sign of a heart problem?
No — most breathlessness is not cardiac. Asthma, COPD, lung infections, anaemia, anxiety and deconditioning account for the majority of cases. Pulmonary embolus, asthma exacerbations and pneumothorax are important acute non-cardiac causes.
Heart-related breathlessness has recognisable features: it often worsens when lying flat (orthopnoea), wakes you in the night gasping (paroxysmal nocturnal dyspnoea), is associated with ankle swelling, comes on with predictable exertion, or is accompanied by an irregular pulse. If any of these apply, a cardiology assessment is worthwhile even if a respiratory cause has already been suggested.
"The word 'heart failure' alarms patients understandably — but it describes a functional state, not a final verdict. Many of my patients with heart failure have completely normal lives with the right treatment. The name is one of medicine's less helpful inventions."
— Dr Sukhjinder Nijjer, Consultant Cardiologist
What is heart failure and is it reversible?
Heart failure is a clinical syndrome in which the heart cannot pump enough blood to meet the body's needs, or can only do so at the cost of high filling pressures. The name is misleading — the heart has not "failed" in the dramatic sense; it is underperforming, and the body responds with fluid retention, breathlessness and fatigue.
Some forms are reversible — alcohol-related cardiomyopathy that improves with abstinence, or tachycardia-induced cardiomyopathy that recovers once the rhythm is controlled. Most chronic heart failure is not fully reversible, but modern treatment can substantially improve symptoms, quality of life, hospitalisations and survival — often dramatically.
Can heart failure be cured?
In selected cases, yes — but more commonly heart failure is controlled rather than cured, similar to high blood pressure or diabetes. Reversible causes — alcohol, untreated arrhythmia, severe valve disease, certain inflammatory conditions — can sometimes be fully treated and the heart muscle can recover.
For most patients, the modern combination of "the four pillars" of heart failure medication — an ACE inhibitor or sacubitril-valsartan, a beta-blocker, a mineralocorticoid antagonist and an SGLT2 inhibitor — plus device therapy where appropriate and lifestyle change provides excellent symptom control and substantially improves life expectancy. The earlier treatment starts, the better the outcome.
Heart failure has a far more positive treatment story than most patients realise. I regularly see patients who arrive quite significantly breathless and limited — sometimes struggling to walk more than a short distance — and within three to six months on the right medication regimen, their echocardiogram shows meaningfully improved heart function and their symptoms are substantially better.
The condition called dilated cardiomyopathy — where the heart muscle weakens and enlarges — can in many cases recover to near-normal function with modern neurohormonal therapy. Getting the diagnosis right is the critical first step. An echocardiogram tells me the ejection fraction and the cause; a cardiac MRI gives even more detail about myocardial scarring and inflammation. From there, the treatment pathway is usually clear — and the results can be remarkable.
NYHA breathlessness classification
Used worldwide to grade exercise limitation in heart failure. Guides treatment decisions and prognosis.
Heart disease present but ordinary physical activity causes no symptoms. Walking, climbing stairs — all normal. Often diagnosed incidentally on echocardiogram.
Comfortable at rest. Ordinary activity — brisk walking, climbing stairs — causes breathlessness or fatigue. Most patients manage daily life with minor adaptations.
Comfortable at rest. Less than ordinary activity causes symptoms. Getting dressed or walking slowly on the flat causes breathlessness. Significant impact on daily life.
Unable to carry on any activity without discomfort. Symptoms present at rest and worsen with any exertion. Requires specialist inpatient or intensive outpatient management.
Why are my ankles swollen?
Ankle swelling has many causes: prolonged standing or sitting, hot weather, pregnancy, varicose veins, certain medications (calcium channel blockers, some painkillers), kidney or liver problems, and venous insufficiency. Heart failure is an important cause but not the most common.
Cardiac ankle swelling is usually bilateral (both legs), worse by evening, pits when you press it, and is accompanied by breathlessness on exertion, breathlessness when lying flat, or fatigue. Sudden one-sided leg swelling needs immediate assessment to exclude a deep vein thrombosis. New, unexplained bilateral ankle swelling with any breathlessness should prompt a cardiac review.
"When patients come to me with breathlessness and ankle swelling that's been put down to 'just getting older', I find it deeply satisfying to identify a treatable cardiac cause and see them return three months later walking normally and sleeping through the night. Heart failure treatment has come a very long way."
— Dr Sukhjinder Nijjer, Consultant Cardiologist
What is the life expectancy with heart failure?
Modern outcomes are much better than older statistics suggest, and life expectancy varies enormously depending on the cause, severity, treatments received and the patient's other health conditions. Some forms of heart failure recover fully; others remain stable for decades with treatment.
With the current four-pillar drug regimen, well-managed mild-to-moderate heart failure carries a five-year survival approaching that of many cancers in remission, and many patients live normal-length lives. The single most important factor in outcome is starting full guideline-directed treatment early and at the correct doses. Outdated prognostic statistics do not reflect today's reality.
Can breathlessness be caused by an irregular heartbeat?
Yes — breathlessness is one of the commonest symptoms of atrial fibrillation, particularly when the heart rate is fast. AFib reduces the efficiency of each heartbeat by around 20–30%, and a sustained fast rate over weeks or months can weaken the heart muscle and cause heart failure — so-called tachycardia-induced cardiomyopathy.
The good news is that this form of heart failure usually reverses once the rhythm or rate is controlled. Any new breathlessness combined with an irregular pulse should be investigated promptly — for the AFib itself, which has implications for stroke risk, and for the impact on heart function.
What tests will diagnose the cause of my breathlessness?
The standard work-up combines an ECG, blood tests including NT-proBNP (a highly sensitive heart failure marker), thyroid function, full blood count and kidney function, a chest X-ray, and an echocardiogram. This combination identifies the cause in the majority of patients.
If the diagnosis remains unclear, further tests may include cardiac MRI, lung function tests, CT coronary angiogram or cardiopulmonary exercise testing (CPET) — the gold-standard test for distinguishing cardiac from respiratory limitation and quantifying true exercise capacity.
Is it normal to feel breathless after COVID?
Persistent breathlessness after a COVID infection is common — affecting up to a fifth of people in the months after acute illness — and most cases improve gradually over 3 to 12 months.
A small proportion of post-COVID breathlessness reflects ongoing lung scarring, myocarditis (heart muscle inflammation), pulmonary embolus, or post-viral autonomic dysfunction (POTS). New breathlessness persisting beyond 12 weeks, or breathlessness with chest pain or palpitations, deserves a cardiac assessment including an ECG, echocardiogram and often cardiac MRI.
What is the difference between heart failure and a weak heart?
The two terms overlap but are not identical. A "weak heart" colloquially means reduced pumping function — what cardiologists call reduced ejection fraction (HFrEF). Heart failure is the clinical syndrome that follows when pumping function is inadequate for the body's needs.
Importantly, heart failure can also occur with a preserved ejection fraction (HFpEF) — the heart pumps normally but is stiff and cannot relax properly, so filling pressures rise and fluid backs up. HFpEF is increasingly recognised, particularly in older patients, women and those with hypertension or obesity. Both forms cause similar symptoms and both have evidence-based treatments.
Related conditions and investigations
This page provides general information for educational purposes and is not a substitute for personalised medical advice. If you are concerned about symptoms, contact a healthcare professional. In a medical emergency, call 999.
Concerned about breathlessness?
Dr Nijjer offers expert assessment of breathlessness at 68 Harley Street, combining cardiac and respiratory investigations to identify the cause and plan the most effective treatment.