Heart Conditions — Emergency
Heart Attacks
Explained
A heart attack is a life-threatening emergency where a coronary artery becomes suddenly blocked. Understanding the signs, the timeline, and the treatments can save your life — or the life of someone close to you.

Understanding the Condition
What is a Heart Attack?
Heart attacks represent a life-threatening emergency where a coronary artery suddenly becomes blocked by a blood clot. The underlying process typically begins with atherosclerosis — the accumulation of cholesterol and inflammatory material within the artery wall. When plaque ruptures, it exposes collagen, triggering rapid clot formation. Because coronary arteries are narrow, even small clots can completely obstruct blood flow.
When blood supply to heart tissue is interrupted, that region stops functioning immediately, producing characteristic symptoms. Rapid intervention to restore blood flow can halt the attack and limit damage.
Notably, patients with minimal plaque disease can experience more severe attacks than those with established coronary disease, because their hearts have not adapted to reduced blood supply. Patients with known coronary narrowing often experience stable angina — discomfort during exertion that resolves with rest — which can be effectively managed with medications that substantially reduce heart attack risk.
"Time is muscle — every minute of arterial blockage destroys more heart tissue. The fastest path to survival is dialling 999 and getting to a Heart Attack Centre."




Recognising a Heart Attack
Symptoms to Act On Immediately
Heart attacks can develop at any time, including during sleep, and are frequently triggered by stress-related blood pressure surges. Most patients describe a sensation of heavy weight on their chest rather than sharp pain.
- Heaviness or tightness across the chest — like a band being tightened around the ribcage
- Pain radiating into the arm, neck, back, or jaw (classically the left arm, but either or both sides)
- Anxiety, sweating, coldness, and clamminess
- Nausea or vomiting
- Brief episodes of brief relief followed by return of symptoms (suggesting temporary arterial reopening)
- Symptoms that intensify over time — a critical warning sign requiring immediate action
Call 999 (UK) immediately and report severe crushing chest pain and your location. If alone, move to your front door and open it before collapsing. Do not drive yourself to hospital.


Immediate Response
The First Steps of Treatment
Immediate hospital assessment is essential for all suspected heart attacks. Every minute of delay increases the damage to heart muscle, so the speed of response is critical.
- 1
ECG & Aspirin — Paramedics perform a 12-lead ECG and administer Aspirin 300mg (ideally chewed) on arrival.
- 2
GTN Spray — Glyceryl trinitrate spray or sublingual tablets dilate coronary arteries. In some cases GTN can halt or slow the attack.
- 3
Heart Attack Centre — In London, patients with specific ECG findings are taken directly to a dedicated Heart Attack Centre staffed 24/7/365.
- 4
Blood Thinners — On arrival, treatment includes high-dose antiplatelet therapy (aspirin with clopidogrel, ticagrelor, or prasugrel) plus heparin injection.
- 5
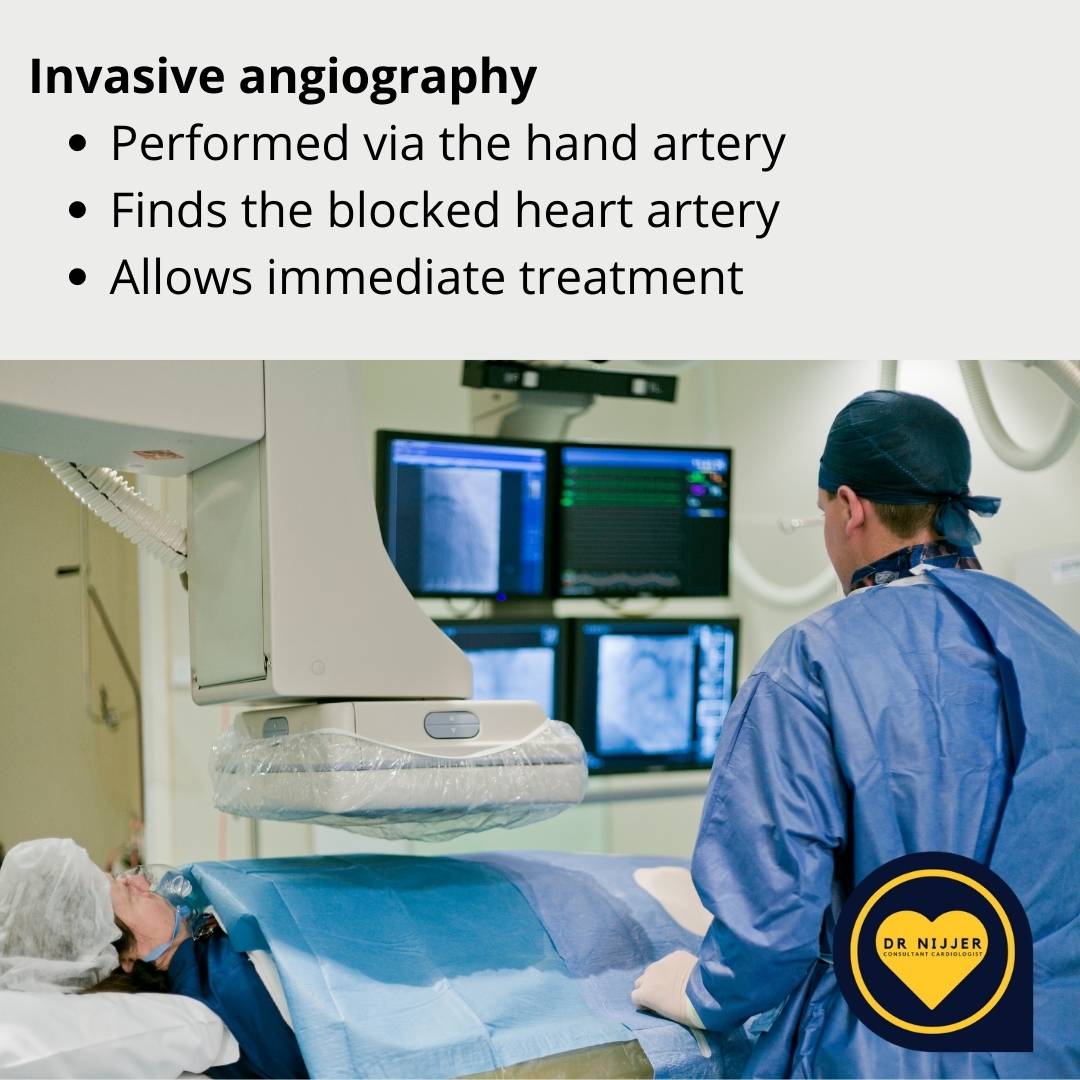
Coronary Angiography — Imaging of the coronary arteries to identify the blockage and guide angioplasty to reopen the artery.
Types of Heart Attack
STEMI & NSTEMI
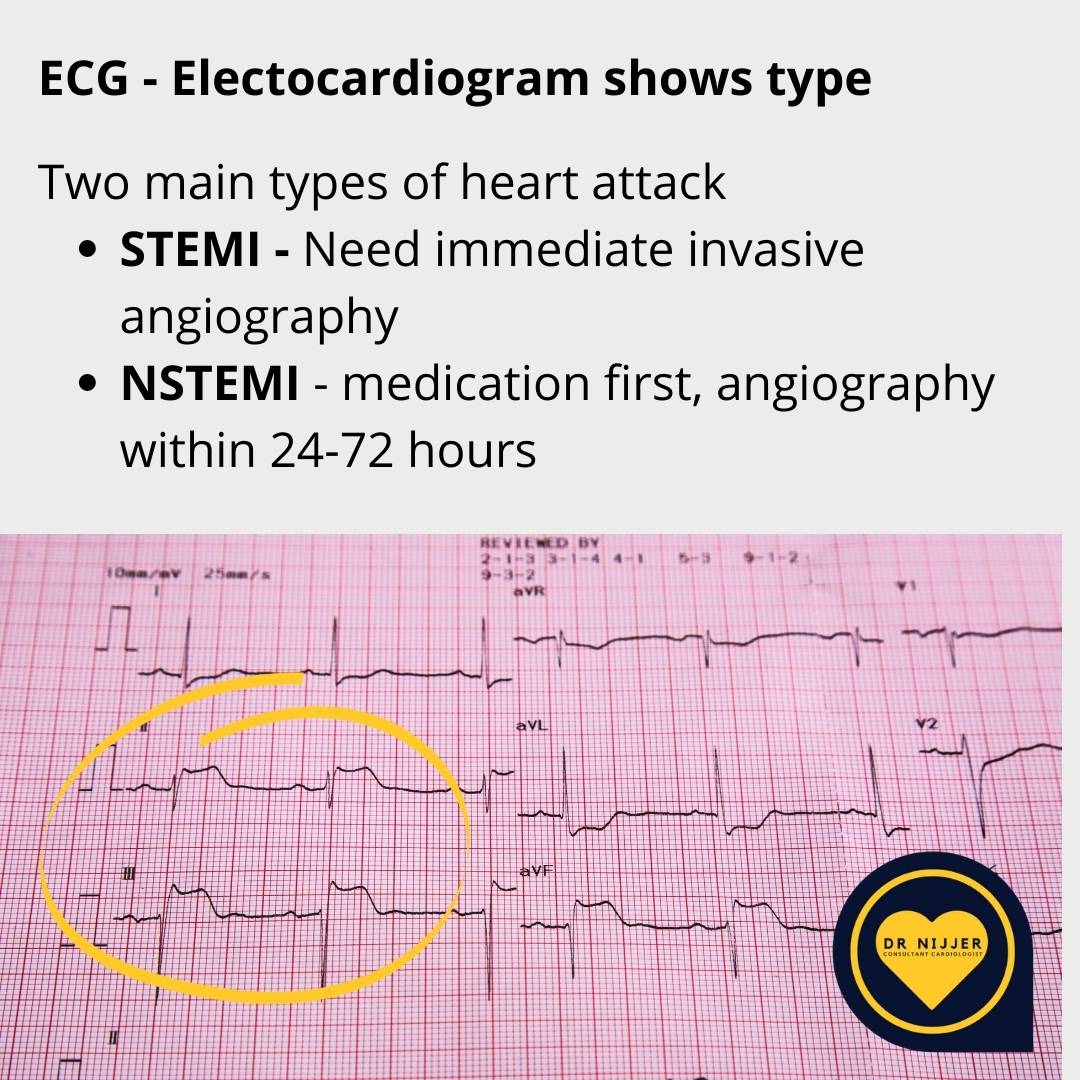
Heart attacks are classified by their ECG appearance, which determines the urgency and type of treatment required.
STEMI
ST-Elevation Myocardial Infarction
STEMI occurs when a coronary artery is completely blocked. The ECG shows a characteristic ST-segment elevation. Heart muscle is being actively destroyed — every second counts.
The Left Anterior Descending (LAD) artery blockage can cause severe scarring and weakened heart function. The Right Coronary Artery (RCA) blockage may disrupt the heart's electrical conducting system, causing Complete Heart Block.
NSTEMI
Non-ST-Elevation Myocardial Infarction
NSTEMI occurs when the artery is partially blocked. Blood markers (troponin) confirm heart muscle damage, though the characteristic ST-elevation is absent on the ECG.
Treatment depends on risk scores and clinical progression. Blood thinners are started immediately. Coronary angiography typically follows within 24–72 hours, guided by the degree of risk.
If Left Untreated
Potential Complications
Untreated heart attacks beyond 12 hours typically result in extensive cardiac damage. Heart muscle that does not receive blood dies and is replaced by scar tissue — this cannot be reversed.
The COVID-19 pandemic demonstrated the consequences of delayed presentation: many patients arrived late with substantial arterial clots that proved significantly harder to treat and with far greater resulting damage.
Early hospital presentation, even if symptoms seem manageable, is always the correct course of action.

Heart Failure
Severe damage to the pumping muscle causes acute lung flooding with fluid, producing severe breathlessness. Long-term heart failure carries a prognosis worse than many cancers.
Arrhythmia
Extensive scarring disrupts electrical conduction. Ventricular tachycardia and ventricular fibrillation are life-threatening without immediate electrical cardioversion.
Valve Disruption
Scarring of valve-supporting structures causes acute mitral or tricuspid regurgitation with sudden pulmonary oedema. Emergency surgical repair carries very high risk.
Cardiac Thrombus
Portions of non-contracting heart wall allow clots to form inside the chamber. These clots can travel to the brain, causing devastating and potentially permanent stroke.
Holes in the Heart
Large areas of dead muscle can rupture, creating a hole in the heart wall. This is a surgical emergency requiring immediate intervention.
Cardiac Arrest
The most serious complication. Ventricular fibrillation causes the heart to stop pumping entirely. Without immediate CPR and defibrillation, death follows within minutes.
After the Event
Medicines Required
After a Heart Attack
Following a heart attack, a combination of medications is prescribed to prevent recurrence, protect remaining heart function, and stabilise the coronary arteries. These medications are typically life-long and should not be stopped without cardiology advice.
Aspirin
Antiplatelet — Blood Thinner
Prescribed to nearly all patients to reduce recurrent heart attack risk. Standard dose is 75mg daily, ideally taken with food. Aspirin can cause stomach ulcers in vulnerable patients and must not be discontinued without cardiologist guidance.
Dual Antiplatelet Therapy
Antiplatelet — Blood Thinner (Combined with Aspirin)
A second antiplatelet agent combined with aspirin significantly reduces recurrent heart attack risk and prevents stent thrombosis — a life-threatening re-blockage of a treated artery.
Clopidogrel (75mg daily) has been used since the late 1990s and is very safe. Ticagrelor (90mg twice daily) is more potent and may cause a harmless sensation of needing a deeper breath. Prasugrel (10mg daily) is the strongest option, reduced to 5mg in patients over 75 or weighing under 60kg.
Duration: at least 12 months following a heart attack or stent placement.
- Clopidogrel
- Ticagrelor
- Prasugrel
Statin
Cholesterol-Lowering — Lipid Modifier
Statins reduce blood cholesterol by modifying a liver enzyme responsible for cholesterol production. Derived originally from Chinese red yeast rice extracts, they have been studied for over 30 years.
Following a heart attack, statins are typically started on the day of the event. They also act to stabilise the ruptured plaque that triggered the attack. Common post-attack choices include atorvastatin (40–80mg) or rosuvastatin.
- Atorvastatin
- Rosuvastatin
- Pravastatin
Beta-Blocker
Heart Rate & Workload Reduction
Beta-blockers calm heart muscle and prevent excessive rate acceleration, reducing cardiac strain after a heart attack. Patients with scarring or reduced function remain on them long-term due to association with prolonged survival.
Side effects can include initial fatigue, cold hands and feet, and occasionally erectile dysfunction in men — all should be reported to Dr Nijjer.
- Bisoprolol
- Carvedilol
ACE Inhibitor
Heart Protection — Blood Pressure
Ramipril and perindopril are blood pressure medications with additional cardiac benefits. They block an abnormal kidney-triggered pathway that worsens heart function, making them a mainstay for all patients with any degree of heart muscle weakness.
Approximately 10% of patients develop a recurrent dry cough, in which case Dr Nijjer may switch to an ARB such as candesartan or irbesartan, which offer similar cardiac benefits without this side effect.
- Ramipril
- Perindopril
- Candesartan (ARB)
Additional Medications
Emerging Therapies — Research-Guided
Emerging evidence supports further medications that improve post-attack heart function. These include extra anticoagulants such as rivaroxaban, and SGLT2-inhibitors originally developed for diabetes (dapagliflozin, empagliflozin, canagliflozin), which have been shown to reduce hospitalisation for heart failure and cardiovascular death.
Dr Nijjer prescribes these based on the latest research evidence.
- Rivaroxaban
- Dapagliflozin
- Empagliflozin
Life After a Heart Attack
Recovery & Cardiac Rehabilitation
Cardiac rehabilitation programmes educate patients on the lifestyle modifications necessary to reduce the risk of further events. Many patients resume normal activity within weeks of a successful angioplasty — a testament to the effectiveness of modern emergency cardiac care.
Dr Nijjer tailors guidance on diet, exercise, and activities specifically to each patient's circumstances, taking into account the extent of any damage, the medications prescribed, and the patient's own goals and lifestyle.
Dr Nijjer's Expertise
Dr Nijjer is the Lead for Cardiac Catheter Laboratories at Hammersmith Hospital and a Principal Investigator in multiple major international studies. He has treated thousands of patients with acute coronary syndromes using the latest angioplasty techniques, including iFR-guided intervention, intravascular imaging, and complex calcium modification.

Related Conditions
Further Reading
Patient Questions
Heart Attack FAQs
The questions Dr Nijjer is asked most often about heart attacks — warning signs, silent MIs, diagnosis, and recovery.
Medically reviewed by Dr Sukhjinder Nijjer, Consultant Interventional Cardiologist (GMC 6103417) · Last reviewed May 2026.
Cardiac catheterisation at Hammersmith Hospital
Dr Nijjer is Lead for the Cardiac Catheter Laboratories at Hammersmith Hospital — one of the UK's busiest interventional cardiology centres. He has treated thousands of patients with heart attacks and coronary disease through angioplasty and stenting.
- Co-developer of iFR pressure wire technology (used globally)
- 150+ peer-reviewed publications on coronary intervention
- Principal Investigator in multiple international guideline-changing studies
- Private consultation same week at One Heart Clinic, Harley Street

Dr Nijjer leads the cardiac cath lab team at Hammersmith Hospital
Call 999 immediately if you suspect a heart attack
Do not drive yourself to hospital. While waiting for the ambulance:
- Chew (do not swallow whole) one 300 mg aspirin, unless you are allergic or have been told not to take aspirin
- Sit or lie in whatever position is most comfortable
- Stay still — exertion increases heart muscle damage
- If you have a GTN spray, use it as instructed by your doctor
A heart attack is not the same as a cardiac arrest. In a cardiac arrest the person collapses and stops breathing normally; begin CPR and use a defibrillator if available.
Questions on this page
- What are the early warning signs of a heart attack?
- Can you have a heart attack without chest pain?
- How are heart attack symptoms different in women?
- Can a heart attack happen during sleep?
- What is a "silent" heart attack?
- How is coronary artery disease diagnosed?
- Can blocked arteries be reversed?
- What does a coronary calcium score tell me?
- Am I at risk if my parent had a heart attack?
- How long does it take to recover from a heart attack?
- What lifestyle changes most reduce heart attack risk?
- Is chest pain after a heart attack normal?
What are the early warning signs of a heart attack?
The classic warning sign is central chest discomfort — pressure, tightness, squeezing or heaviness — lasting more than 15 minutes and often radiating to the left arm, jaw, neck, back or upper abdomen. It is commonly accompanied by breathlessness, cold sweat, nausea, light-headedness or a sense of impending doom.
In many people, warning signs appear days or even weeks before the heart attack itself, in the form of new-onset angina or a clear change in an existing angina pattern — coming on more easily, lasting longer, less responsive to rest. Do not dismiss a new or changing pattern of exertional chest discomfort.
Can you have a heart attack without chest pain?
Yes — around 20% of heart attacks present without classic chest pain. This is particularly common in older patients, women, people with diabetes, and those with chronic kidney disease.
Atypical presentations include severe unexplained breathlessness, sudden profound fatigue, indigestion that will not settle, jaw or back pain, fainting, or just an overwhelming sense that something is wrong. If you have cardiovascular risk factors and develop any new, severe or unfamiliar symptom with no obvious explanation, treat it as cardiac until proven otherwise.
"I've spent much of my career as an interventional cardiologist, which means I've seen the full spectrum of heart attacks — from those caught within minutes to those where delay made a real difference. The message I want every patient to take away is simple: if it feels wrong, call 999. Paramedics can begin treatment on the way to hospital, and every minute genuinely matters."
— Dr Sukhjinder Nijjer, Consultant Interventional Cardiologist, Harley Street
How are heart attack symptoms different in women?
Women are more likely than men to have atypical heart attack symptoms — breathlessness, fatigue, nausea, jaw or upper-back pain, dizziness — without dramatic central chest pain. Women are also more likely to dismiss these symptoms or be misdiagnosed, which contributes to worse outcomes.
A heart attack in a woman can present as profound unexplained fatigue in the weeks before the event, then breathlessness or upper-back pain on the day. Heart disease is the leading cause of death in UK women, and women's heart attacks are too often missed because they don't look like the textbook picture. See the women and heart disease FAQ for more.
Can a heart attack happen during sleep?
Yes — heart attacks can occur at any time, including during sleep. There is actually a peak in incidence in the early morning hours (roughly 4 am to 10 am), driven by a natural surge in stress hormones, heart rate and blood pressure as you wake.
A heart attack during sleep may wake you with chest discomfort, breathlessness or a sense of dread. Untreated sleep apnoea is an important and under-recognised risk factor for nocturnal heart attacks and arrhythmias, so heavy snoring with daytime sleepiness deserves investigation.
I've been lead of the cardiac catheterisation laboratories at Hammersmith Hospital for many years, and in that time I've treated thousands of patients with heart attacks. The single most important message is this: do not wait. The phrase 'time is muscle' is completely accurate — every minute without blood flow costs heart muscle that cannot be replaced.
When a patient arrives with a heart attack, our team opens the blocked artery with an angioplasty and stent as rapidly as possible — typically within 90 minutes of the call for help. In complex cases I use iFR pressure wire assessment to guide which vessels need treatment, and intracoronary imaging to ensure the stent is optimally placed. The outcomes from modern heart attack treatment are genuinely remarkable compared to even a decade ago.
Recovery after a heart attack — what to expect
What is a "silent" heart attack?
A silent heart attack is one that occurs with little or no recognisable symptoms at the time, and is only discovered later — often when an ECG, echocardiogram or scan picks up scar tissue in the heart muscle. They account for around 1 in 5 heart attacks in the UK.
Silent heart attacks are commonest in people with diabetes (whose nerve signalling can blunt pain perception), the elderly, and women. They carry the same long-term risk of complications as a recognised heart attack — heart failure, further events, arrhythmia — which is why finding them and treating the underlying coronary disease matters.
How is coronary artery disease diagnosed?
The first-line test in the UK for suspected coronary artery disease is a CT coronary angiogram under NICE guidance — a quick, non-invasive scan that shows the coronary arteries in detail and identifies narrowings or calcium build-up.
If the CT shows significant disease, the next step is usually an invasive coronary angiogram, performed via the wrist or groin, often with pressure-wire assessment (iFR or FFR) to decide which narrowings actually need stenting. Other useful tests include stress echocardiography and cardiac MRI for assessing how the heart muscle behaves under load.
"The iFR pressure-wire technique is something I've been closely involved in developing and using throughout my career. What it allows us to do is look at a narrowing on an angiogram and know — definitively — whether it is actually limiting blood flow to the heart. That matters enormously, because treating a narrowing that isn't causing a problem adds risk without benefit."
— Dr Sukhjinder Nijjer
Can blocked arteries be reversed?
Heavily calcified, mature plaques cannot be fully reversed, but their progression can be halted and even modestly regressed with aggressive risk-factor control. The strongest evidence is for intensive cholesterol lowering with high-dose statins, sometimes combined with ezetimibe or a PCSK9 inhibitor, which can shrink the soft, dangerous component of a plaque.
Equally important is keeping blood pressure tight, stopping smoking, exercising regularly, controlling diabetes and following a Mediterranean-style diet. The goal is not just to reduce plaque size but to make it more stable — stable plaques rarely rupture and cause heart attacks.
What does a coronary calcium score tell me about my heart?
A coronary calcium score is a quick, low-dose CT scan that measures calcified plaque in your coronary arteries. The result — your Agatston score — quantifies the amount of calcium and translates into a 10-year risk of heart events.
A score of 0 means no detectable calcium and a very low risk over the next decade. A score over 100 suggests significant plaque burden and usually triggers more aggressive prevention. A calcium score is most useful in middle-aged adults with intermediate risk, where the decision about starting a statin is genuinely uncertain — it makes that decision evidence-based rather than guess-based.
Am I at risk of a heart attack if my parent had one?
Yes — a family history of early heart disease (a first-degree relative with a heart attack before age 55 in men or 65 in women) roughly doubles your risk and is treated as an independent risk factor by NICE. The earlier and the closer the family member, the stronger the signal.
This does not mean a heart attack is inevitable, but it does mean you should be assessed earlier and more thoroughly than average. A baseline assessment in your 30s or 40s — including blood pressure, full lipid profile, Lp(a), glucose, and often a calcium score — can refine your individual risk and guide early prevention.
How long does it take to recover from a heart attack?
Most people are discharged from hospital within 2 to 4 days of an uncomplicated heart attack, return to light activity within a week or two, and can usually return to desk-based work within 4 to 6 weeks. Recovery from a larger heart attack with significant muscle damage takes longer.
Cardiac rehabilitation, started within a few weeks of discharge, halves the risk of dying in the following decade and is one of the most under-used treatments in cardiology. Most patients should also expect to take long-term medication — typically a statin, an antiplatelet, a beta-blocker and an ACE inhibitor or ARB.
"Cardiac rehabilitation is genuinely one of the best things a patient can do after a heart attack, and it's one of the most under-used. The combination of supervised exercise, education and risk-factor support halves the risk of dying in the subsequent decade. I always encourage patients to take up the offer — it's not about restriction, it's about rebuilding."
— Dr Sukhjinder Nijjer
What lifestyle changes most reduce heart attack risk?
The four interventions with the largest individual effect, in order of magnitude, are: stopping smoking (cuts cardiovascular risk by around 50% over a few years), treating high blood pressure, lowering LDL cholesterol with statins where indicated, and regular physical activity (150 minutes a week of moderate-intensity exercise).
A Mediterranean-style diet, weight control, limiting alcohol to under 14 units a week and managing stress add further benefit. Combined, these changes can reduce the risk of a heart attack by 70–80% — a much bigger effect than any single medication. More detail on the heart health and lifestyle FAQ page.
Is chest pain after a heart attack normal?
Some chest discomfort in the days after a heart attack — particularly a brief sharp pain or a sense of bruising — can come from the procedure site (if a stent was inserted) or from pericarditis (inflammation of the sac around the heart, sometimes called Dressler's syndrome).
Recurrent pressure-type chest pain similar to the original heart attack should be treated as a new event and trigger a 999 call. Re-blockage of a stent, a new narrowing, or a missed second lesion can all occur. Do not try to assess this at home — get reviewed immediately.
Related conditions and treatments
Trusted external resources
This page provides general information for educational purposes and is not a substitute for personalised medical advice, diagnosis or treatment. In a medical emergency, call 999. Last reviewed May 2026; next review due May 2027.
Concerned about your heart health?
Dr Nijjer offers expert cardiology consultations at 68 Harley Street and across four London clinic sites. Whether you have had a heart attack or are concerned about your risk, arrange an appointment today.