Diagnostic Test
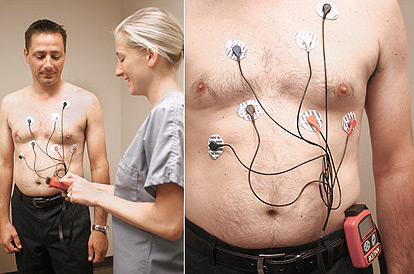
ECG (Electrocardiogram)
A resting ECG records the heart's electrical activity from twelve different angles, providing an instant snapshot of heart rhythm, rate, and conduction. Painless and performed in minutes, it is often the essential first investigation for any cardiac symptom.
Read more →